

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nosocomial infections caused by Acinetobacter baumannii and that exhibit resistance to virtually all antimicrobial agents assayed in vitro have rapidly increased in recent years (1-3). Fortunately, these multidrug resistant strains have retained susceptibility to colistin, which is a polymyxin-family antimicrobial agent that was used several generations ago. This finding of retained colistin susceptibility has led to widespread reintroduction of the agent (4). Several studies have reported on the therapeutic and adverse effects associated with colistin use, and these studies have generally reported a favorable profile (4-6). However, there have been few well-designed studies that have evaluated whether the reintroduction of colistin has a meaningfully impact on the outcomes of patients with multidrug resistant (MDR) A. baumannii infections.
In Korea, MDR A. baumannii strains have been isolated since the late 1990s. Korean clinicians initially did not have access to colistin and they were forced to use less-than-ideal agents such as carbapenems, ampicillin-sulbactam, piperacillin-tazobactam, cephalosporins or fluoroquinolones despite their poor performance on in vitro susceptibility assay. Since parenteral colistin became available in late 2006, the agent has become the firstline treatment for MDR A. baumannii infection.
The main objective of our study was to investigate whether the reintroduction of colistin improved the survival outcomes of patients with MDR Acinetobacter spp. bloodstream infections. We also compared the outcomes between in patients who were treated with colistin and in those who were treated without colistin.
MATERIALS AND METHODS
Study design and population
The microbiology laboratory database was electronically queried to identify all the blood cultures that were positive for Acinetobacter spp. from the patients admitted between June 2000 and August 2007 at Asan Medical Center (AMC), which is a 2,200-bed tertiary care center in Seoul, Korea. The eligible subjects were all hospitalized patients with a positive blood culture for MDR Acinetobacter spp.; and they met the US Centers for Disease Control and Prevention criteria for health care-associated infection (7). For the patients who had more than one episode of Acinetobacter spp. bacteremia, only the first episode was considered. The patients with polymicrobial bloodstream infection were included.
The colistin group was identified as the patients who were treated with parenteral colistin with or without other antimicrobials. The patients in the non-colistin group were treated with either single or combination antimicrobials that the Acinetobacter spp. isolates were not susceptible to according to in vitro testing.
We excluded the patients younger than 12 months and the patients who could not receive the required treatment measures in addition to systemic antimicrobial therapy. Patients were excluded if they received fewer than 72 hr of antimicrobial therapy (8). Patients were also excluded if they were treated late, and this was defined as receiving the first dose of antibiotics more than 24 hr after the pathogen had been identified and the susceptibility testing had been completed.
We compared the 30-day in-hospital mortality as well as the clinical variables that could influence mortality among the colistin treated and non-colistin-treated patients. In addition, we performed a subgroup analysis of the patients who received colistin as early empiric treatment until the final bacteriologic evaluation was available. These patients received colistin within 48 hr after the onset of bacteremia, but before MDR Acinetobacter spp. was identified.
Colistin administration
All the patients in the colistin group received colistimethate sodium methanesulfonate (SteriMax Inc., Ontario, Canada). They received colistin base via parenteral delivery at a dose of 2.5-5.0 mg/kg (75,000-150,000 IU/kg) per day divided into two or three doses (6). Dosage adjustments were made according to the creatinine clearance in the patients with renal failure based on the recommendations of prior reports (4).
Microbiological methods
Standard media and techniques were used for bacterial isolation and identification. Identification and antimicrobial susceptibility testing for all the antimicrobial agents except colistin was performed using the MicroScan automated broth microdilution method with a MicroScan NegCombo Panel Type 32 (Dade Behring, Sacramento, CA, USA). The breakpoints were those defined by the Clinical and Laboratory Standards Institute (CLSI) (9). Intermediate sensitivity was considered resistance. Susceptibility to colistin was tested by means of the agar dilution method and a susceptible isolate was defined as having a minimal inhibitory concentration (MIC) ≤ 2.0 µg/mL according to the CLSI guidelines (9). Pseudomonas aeruginosa ATCC 27853 was used as a quality control strain (9).
Data collection
We collected all the available medical information including age, gender, the length of the intensive care unit (ICU) stay, the medication history, underlying diseases and the calculated Charlson's comorbidity index. Data on acute organ failure, the Acute Physiological and Chronic Health Evaluation II score (APACHE II score) and the Pitt bacteremia score on the day of bacteremia were also collected. Information regarding the suspected or proven portal of entry, the presence of polymicrobial bacteremia, the duration of antibiotic administration and the presence of other antimicrobial agents were also collected. In addition, laboratory data such as the complete blood counts, renal and liver function tests and the C-reactive protein level were collected.
Operational definitions
We defined MDR Acinetobacter spp. as strains that demonstrated in vitro resistance to all of the following antimicrobial agents; penicillins (ampicillin, ampicillin-sulbactam, ticarcillin-clavulanate, piperacillin-tazobactam); cephalosporins (ceftriaxone, cefotaxime, ceftazidime, cefepime); carbapenems (imipenem, meropenem); aminoglycosides (tobramycin, gentamicin, amikacin); fluoroquinolones (ciprofloxacin, levofloxacin); and monobactam (aztreonam).
Acute organ system failure (i.e., cardiovascular, respiratory, renal, hematologic or central nervous system) was defined using the definitions of Zimmerman et al. (10). Acute liver failure was defined as the appearance of encephalopathy within 2 weeks of developing jaundice.
The diagnosis of pneumonia, intra-abdominal infection, urinary tract infection, central venous catheter-related blood stream infection, skin and soft tissue infection and primary bacteremia were based on the guidelines issued by the Centers for Disease Control and Prevention (7).
Normal renal function was defined as a serum creatinine level of 1.3 mg/dL or lower (8). Deterioration of renal function was defined as an increase of more than 50% in the baseline creatinine level to a value higher than 1.3 mg/dL or a decline in renal function that required hemodialysis (8). Irreversible renal dysfunction was defined as failure of the serum creatinine level to return to baseline after discontinuation of the antimicrobials. The baseline creatinine level was defined as the creatinine level on the first day of administering antimicrobial agents.
Outcome measures
The primary outcome measure was the overall in-hospital mortality at 30 days from the day on which bacteremia was first detected. Because colistin was withdrawn in the 1970s largely due to its association with acute renal failure, we also followed the effects of colistin treatment on the renal function during treatment as a secondary end point. When analyzing the outcomes of renal dysfunction, we excluded the patients who were already receiving renal replacement therapy before undergoing antibiotic treatment.
Statistical analysis
Categorical variables were compared by the chi-square test or Fisher's exact test. For continuous variables, we used the Mann-Whitney U test. The data is reported as the median (range) and the odds ratio with the 95% confidence intervals. All the tests were two-tailed, and statistical significance was set for P values < 0.05. Multivariate analysis was conducted to determine the adjusted odds ratios for the predictors of mortality. Variables with a P value < 0.05 on the univariate analysis were considered for inclusion in a logistic regression model. We chose a representative variable if several variables with P values < 0.05 were seemed to have similar clinical relevance. Colistin treatment was entered into the regression model irrespective of these requirements as it represented the principal variable under investigation. All the statistical analyses were performed with SPSS 12.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
Study population
Thirty-six patients who were treated with colistin for MDR Acinetobacter spp. bacteremia were identified. One patient was an infant ≤ 12 months of age, and 2 patients were excluded due to an insufficient duration of colistin therapy. Another two patients were excluded because they began colistin therapy after identifying the MDR Acinetobacter spp. infection. Forty patients were included in the non-colistin group. One advanced malignancy patient was excluded because he refused drainage of an intraperitoneal abscess and instead requested hospice care. Finally, 31 patients were included in the colistin group and 39 in the non-colistin group.
Colistin susceptibility tests were performed using the stored blood isolates in the laboratory. All 31 Acinetobacter spp. isolates derived from the colistin group were stored. However, for the case of the non-colistin group, not all the isolates had been stored in the laboratory, so susceptibility tests could be performed to only 17 of 39 isolates. All 48 tested Acinetobacter spp. strains were susceptible to colistin as verified by an MIC for colistin ≤ 2 µg/mL, which is consistent with the CLSI guidelines (9). The MIC50 was 0.190 µg/mL and the MIC90 was 0.380 µg/mL in both groups.
Demographic and clinical characteristics
Table 1 shows the basic demographic data and clinical features of our cohort, including several clinical severity indices. There was no significant difference between colistin and non-colistin groups. The two groups were similar with respect to the treatment duration and the utilization of combination therapy. Twenty of 31 patients (64.5%) were treated with colistin within 48 hr after the onset of bacteremia and they were regarded as the patients who received appropriate early empirical colistin therapy. Eleven patients (35.5%) in the colistin group received combination antimicrobial therapy (7 patients received carbapenems, 4 received other combinations). Three patients (9.7%) received combined therapy with antimicrobial preparations that included sulbactam such as ampicillin-sulbactam or cefoperazone-sulbactam.
In the non-colistin group, commonly prescribed antimicrobials included carbapenems (59.0%), fluoroquinolones (51.3%) and piperacillin-tazobactam (28.2%) as part of either single or combination therapy. Antimicrobials that included sulbactam were administrated to 7 patients (18.0%) in the non-colistin group, which was not significantly different from the frequency of sulbactam-containing preparations in the colistin-treated group (P = 0.49).
Primary outcome
The treatment outcomes are depicted in Table 2. Eleven of 31 patients (35.5%) of the colistin group and 15 of 39 patients (38.5%) of the non-colistin group died within 30 days after the onset of bacteremia (P = 0.80) despite the fact that only the patients in the colistin group had received microbiologically appropriate treatment. All the causes of mortality were recorded as septic shock or multi-organ dysfunction syndrome.
In the colistin group, 11 patients were administered another antimicrobial agent simultaneously in addition to colistin and 20 patients received colistin monotherapy. The 30 day in-hospital mortality was 45.5% (5 of 11) in patients who received combination therapy and 30.0% (6 of 20) in those who received colistin alone, and there was no significant difference (P = 0.45).
The twenty patients who were treated empirically with colistin within 48 hr from the onset of bacteremia were also studied as part of a subgroup analysis. All the patients in the non-colistin group had been administered an antimicrobial agent at the time bacteremia developed. The demographic and clinical characteristics between this early appropriate colistin treated subgroup (n = 20) and the non-colistin treated group (n = 39) were not significantly different (data not shown). Overall 30 day mortality was not significantly different. Seven of 20 patients (35.0%) in the subgroup of early empirical colistin therapy and 15 of 39 patients (38.5%) in the non-colistin-treatment group died within 30 days (P = 0.80).
Secondary outcome
Renal dysfunction was evaluated for the 20 patients in the colistin group and for the 35 patients in the non-colistin group. When analyzing the outcomes of the patients with renal dysfunction, we excluded the patients who were already receiving renal replacement therapy before the administration of colistin or other antimicrobials. As a result, 11 of 31 patients (35.5%) were excluded in the colistin group, but only 4 of 39 patients (10.3%) were excluded in the non-colistin group and there was a significant difference (P = 0.02). The basic demographic and clinical characteristics were not significantly different between the 20 patients in the colistin group and the 35 patients in the non-colistin group (data not shown) except that neutropenia was more frequent in the non-colistin group (0% vs 20.0%, respectively, P = 0.04). Ten of the 20 patients (50.0%) in the colistin group and 10 of the 31 patients (28.6%) in the non-colistin group developed renal insufficiency after antimicrobial treatment (Table 2), but there was no statistically significant difference (P = 0.11). Irreversible renal insufficiency developed more frequently in the colistin group, but this difference did not reach stostical significance (30.0% vs 14.3%, respectively, P = 0.18).
Mortality risk factor analysis
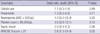
Among the 70 patients enrolled, 26 died and 44 had survived 30 days from the onset of bacteremia. The factors that might predict mortality were analyzed. Univariate analysis was performed initially; the significant factors from this analysis included neutropenia, a platelet count ≤ 80,000/µL, pneumonia as a portal of entry, the intensive care unit (ICU) stay, septic shock, the presence of organ failures and a high score for either the APACHE II score or the Pitt bacteremia score. Multivariate analysis (Table 3) found that an APACHE II score ≥ 21 was the only significant factor that could predict the overall 30 days mortality (P = 0.02). Colistin treatment itself was not an independent risk factor of mortality.
DISCUSSION
Interest in A. baumannii infection has been growing and maily because of the emergence of multidrug-resistant strains (11). Since many A. baumannii strains are now susceptible only to a single known agent, terms such as 'colistin-only-susceptible' or 'polymyxin-only-susceptible' are now commonly used. The difficulty in treating these new drug resistant A. baumannii strains has led to the reintroduction of colistin without evidence of the efficacy beyond in vitro assays and historical experience (4, 6). When colistin was developed and introduced in the 1950s, the contemporary procedures for new drug development and clinical approval were not yet in place (5). The past regulations were considerably looser than the current requirements, and there are substantial gaps in the available knowledge regarding the basic pharmacology of this antibiotic (6). Several studies have been performed in recent years in order to reevaluate the efficacy and safety of colistin; the majority of these studies found that colistin is clinically effective with acceptable adverse effects (12, 13).
However, the available literature does not conclusively demonstrate better outcomes among the patients treated with colistin for MDR A. baumannii infections. The previous studies have lacked control group because it was ethically unacceptable to withhold colistin from patients with MDR A. baumannii infection; colistin was known to be the only in vitro susceptible agent (6).
Second, the previous studies usually included all the subjects with various health care-associated infections such as pneumonia, intra-abdominal infection and surgical wound infection. A. baumannii is commonly colonized from endotracheal tubes, surgical drains and open skin wounds in hospitalized patients. It is quite difficult to differentiate true infection from colonization unless A. baumannii was isolated from blood or other sterile body fluids (14), and thus there is concern about overdiagnosing MDR A. baumannii infection. For overcoming this limitation, we need abundant clinical reports of colistin based on only bloodstream infection (15).
It is not an established conclusion that appropriate antimicrobial treatment actually improves the survival of the patients with an drug resistant A. baumannii bloodstream infections. Some recent studies have revealed that inappropriate antimicrobial treatment was a independent risk factor of mortality (16, 17). However, several studies have demonstrated that appropriate antimicrobial did not improve survival (15, 18, 19). Other studies failed to prove that appropriate treatment was an independent risk factor for mortality (20, 21).
Our findings indicated that there was no improvement of the 30 day overall mortality for patients treated with colistin when it was used as the sole microbiologically appropriate agent. An association with mortality was not revealed for the subgroup of patients who received colistin within 48 hr after the onset of bacteremia. Although this result is somewhat surprising, there are several explanations.
First, although A. baumannii may be quite resistant to most antimicrobials, the available evidence suggests it is not a highly virulent pathogen (22, 23). The prognosis for bacteremia caused by A. baumannii is controversial. On one hand, its clinical relevance is under question (24). Blot et al. (25) reported that the calculated attributable mortality rate of A. baumannii bacteremia was only 7.8% and they concluded that in critically ill patients it was not associated with increased mortality. On the other hand, several clinical reports have offered opinions that are contrary to this position (13, 26).
Second, by studying only the cases with demonstrated bacteremia, we preselected the more severely ill patients than was described in the previous reports. In our study, the median APACHE II score of the colistin-treated group was 20 (range: 8-45) and the median Pitt bacteremia score was 3 (range: 0-14). We suggest that several host factors, including severe co-morbid disease, multiple organ failure and impaired immunity, may be more important determinants of the outcome than purely the susceptibility to antimicrobial agent (14, 15, 18, 25). Indeed, the results of our multivariate analysis showed that the APACHE II score was the single important factor most highly associated with mortality.
Third, it could be related to the efficacy of colistin. The efficacy of colistin is not yet fully accepted. Several experimental models have provided disappointing results about the efficacy of colistin (27, 28). It is also possible explanation that the in vivo effects of colistin do not correlate well with the results of in vitro testing (23).
We observed that deterioration of renal function is more commonly developed in patients treated with colistin (50.0% vs 28.6%, respectively), but this result was not statistically significant (P = 0.11). It was possible to include only 20 patients in the colistin group and 35 patients in the non-colistin group in the analysis for the development of renal insufficiency. Patients were excluded because receiving renal replacement therapy before undergoing antimicrobial therapy was more common in the colistin group than that in the non-colistin group (35.5% vs 10.3%, respectively, P = 0.01). This difference could be explained by the prevalence of renal failure at the time of sepsis (38.7% in the colistin group vs 20.5% in the non-colistin group, P = 0.12) and more active and earlier stage application of continuous renal replacement therapy at the ICU has been done in the recent years.
The secondary outcome analysis was complicated by the presence of several confounding factors, including hemodynamic instability, multi-organ system failure, injection of radiocontrast dye for imaging studies and the co-administration of other nephrotoxic therapeutic agents such as vancomycin, aminoglycosides and diuretics. Actually, 38 (69%) of the 55 patients included in the analysis were treated in the ICU and 22 patients (40%) were in septic shock when bacteremia developed.
The limitations of the present study include its relatively small size and retrospective nature, and this limits the ability to draw definitive conclusions about the efficacy and safety of colistin. Furthermore, these findings should not be broadly generalized beyond the conditions studied herein. For example, it remains to be seen whether colistin is effective for treating non-bloodstream infections and less severely ill patients. In addition, our study only examined the all-cause 30 day mortality, and other end-points could conceivably have been affected by colistin treatment.
More clinical data obtained via controlled clinical trials is needed to confirm our preliminary conclusions. Other reports from physicians with similar experiences due to the geographic limitations of colistin's availability may also be extremely useful (29, 30).
In summary, our study suggests that the reintroduction of colistin, which is the sole microbiologically appropriate agent for this bacterium, does not improve the overall 30 day in-hospital mortality in patients who have a MDR Acinetobacter spp. bloodstream infection. A high APACHE II score was the only significant risk factor that could predict mortality. Our results suggest that the clinical severity of patients may be more important than concordant antimicrobial treatment for determining the outcome of a MDR Acinetobacter spp. bloodstream infection.


 XML Download
XML Download