

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The number of people with diabetes is increasing due to population growth, aging, urbanization and the increasing prevalence of obesity and physical inactivity. According to the World Health Organization (WHO), the prevalence of diabetes for all age-groups worldwide was estimated to be 2.8% in 2000 and 4.4% in 2030 (1). Estimation of the prevalence of earlier stages of chronic kidney disease (CKD) in the US population and ascertainment of trends over time is central to disease management and prevention planning, particularly given the increased prevalence of obesity and diabetes (2). To prevent this increase, screening for CKD and early intervention are necessary. In diabetic patients, the early detection of diabetic nephropathy has focused on the measurement of urinary albumin excretion rate. The elevated urinary albumin excretion rate within microalbuminuric level (30-299 mg/24 hr or a spot urine albumin-to-creatinine ratio of 30-299 mg/g) allows the detection of patients with an increased risk for the development of overt diabetic nephropathy with persistent macroalbuminuria. Moreover, impaired renal function may be present even in patients with normal urinary albumin excretion rate (3). Gold standard procedures for glomerular filtration rate (GFR) measurement, based on the clearance of 51Cr-EDTA or iohexol, are impractical in clinical settings and for larger research studies.
Cystatin C, a cysteine protease inhibitor, is freely filtered by the renal glomeruli, metabolized by the proximal tubule and identified as a promising marker of renal failure (4). Cystatin C is produced at a constant rate by nucleated cells and released into bloodstream with a half-life of 2 hr. Its concentration is almost totally dependent on GFR. Other studies have demonstrated that serum cystatin C is an early renal marker in diabetic patients (5-7), but not all studies have done so (8).
Thus, we explored the possibility of the cystatin C levels of serum and urine as markers of early renal impairment in normoalbuminuric patients with diabetes. We also evaluated the relationship of albuminuria and serum/urine cystatin C.
MATERIALS AND METHODS
Patients
We retrospectively studied the samples of serum and urine from 335 patients with type 2 diabetes who visited our hospital between January 2008 and October 2009. We recorded confidential information of name, age, gender, race, height, weight and history of renin-angiotesin system inhibitors or antihypertensive medication. Because thyroid function could affect the levels of cystatin C (9), we excluded the patients with thyroid disease, or taking the medication due to thyroid disease in 6 months. We also excluded patients with uncontrolled hypertension making an effect on albuminuria.
The cystatin C levels of serum and urine were measured by the latex agglutination test (Modular P800, Roche, Diagnostics, Mannhein, Germany). The eGFR level was calculated using the Modification of Diet in Renal Disease (MDRD) formula: MDRD = 186 × (serum creatinine [mg/dL])-1.154 × age-0.203 (10). A correction factor of 0.742 was used for women. The eGFRcys level was calculated by the Chronic Kidney Disease Epidemiology (CKD-EPI) equation: eGFR = 127.7 × (cystatin C in mg/L)-1.17 × (age in years)-0.13 × (0.91 if female) (11). Patients were divided into 3 groups according to their urinary albumin concentration: those with normoalbuminuria (n = 210), those with microalbuminuria (n = 83) and those with macroalbuminuria (n = 42). Moreover, normoalbuminuric patients were subdivided according to eGFR calculated by the MDRD formula: those with ≥ 60 mL/min/1.73 m2 (n = 181) and those with GFR < 60 mL/min/1.73 m2 (n = 29).
Statistical analysis
In statistical analysis, SPSS for Windows (version 13.0) were used. Data are presented as mean ± SD for normally distributed values. Differences between the groups were analyzed by ANOVA, followed by the Bonferroni's test for normally distributed values and by the Kruskal-Wallis test, as well as the Dunn's test for non-parametric values. Pearson's correlation coefficient was employed to test the correlations between different variables. Before testing correlations, all non-normally distributed values were log-transformed to better approximate normal distributions. After correlation analysis, stepwise multiple linear regression was performed with the variables to find the factor that effects the cystatin C levels of serum and urine. Receiver operating characteristics (ROC) analysis was employed to calculate the area under the curve (AUC) for the cystatin C levels of serum and urine to find the best cutoff values for identifying renal impairment in diabetic patients. Logistic regression was performed to find the predicting factors for renal impairment in normoalbuminuric patients. All results were considered significant if P < 0.05.
RESULTS
Patient characteristics
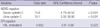
Patients were categorized into 3 groups depending on their urinary albumin excretion evaluated using the urine albumin/creatinine ratio (ACR) (mg/g creatinine): the macroalbuminuric, microalbuminuric and normoalbuminuric groups. The baseline characteristics of the subjects are shown in Table 1. There were no significant differences in age and sex between the 3 groups. However, eGFR was significantly lower in the macroalbuminuric group (44.9 ± 26.6) than in the microalbuminuric (76.0 ± 27.8) and normoalbuminuric groups (84.6 ± 23.3) (P < 0.001). A high ACR was associated with antihypertensive agents, renin-angiotensin system (RAS) inhibitors, lipid lowering agents, high HbA1C/glucose, low eGFR and high triglycerides (Table 1).
Differences in the cystatin C levels of serum and urine according to albuminuria
The levels of cystatin C in serum showed stepwise increase with albuminuric levels (P < 0.001, P = 0.013, respectively) (Table 1, Fig. 1). Serum cystatin C was significantly different according to their albuminuria (normoalbuminuria vs microalbumiuria, P < 0.01; microalbumiuria vs macroalbuminuria, P < 0.001; normoalbuminuria vs macroalbuminuria, P < 0.001) (Table 1, Fig. 1A). The level of urine cystatin C also showed stepwise increase with albuminuric level (normoalbuminuria vs microalbumiuria, P < 0.05; microalbumiuria vs macroalbuminuria, P < 0.001; normoalbuminuria vs macroalbuminuria, P < 0.001) (Table 1, Fig. 1B).
Parameters related to the cystatin C levels of serum and urine in diabetic patients
The correlations between the log-transformed cystatin C levels of serum and urine and the albumin creatinine ratio were analyzed in all diabetic patients. The serum level of cystatin C was found to directly correlate with albuminuria (r = 0.555, P < 0.001). The urine level of cystatin C also positively correlated with albuminuria (r = 0.500, P < 0.001). In Pearson's correlation analysis, the serum level of cystatin C was related to age, ACR, creatinine, eGFR, C-reactive protein (CRP), high-density lipoprotein and systolic blood pressure; and the urine level of cystatin C was related to ACR, HbA1C, creatinine, GFR, CRP and glucose. We performed a stepwise multiple regression analysis with these factors. The serum level of cystatin C was related to CRP, ACR and GFR, and the urine level of cystatin C was related to triglyceride, age, eGFR and ACR.
Differences in the cystatin C levels of serum and urine according to eGFR in the normoalbuminuric group
Table 2 presents the clinical characteristics of 210 patients with normoalbuminuria according to their eGFR. The patients with eGFR < 60 mL/min/1.73 m2 (n = 29, 14%) by the MDRD equation were older, had lower high density lipoprotein levels (40.3 ± 12.2 vs 46.9 ± 12.4 mg/dL, P = 0.008), had higher cystatin C levels of serum (1.21 ± 0.42 vs 0.86 ± 0.18 mg/L, P < 0.001) and urine (0.11 ± 0.11 vs 0.06 ± 0.45 mg/L, P = 0.013) than those with eGFR ≥ 60 mL/min/1.73 m2. However, there were no significant differences in ACR.
ROC Analysis of cystatin C levels of serum and urine
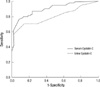
ROC analyses were performed to define the diagnostic profile of the serum and urine levels of cystatin C for detecting eGFR < 60 mL/min/1.73 m2 among subjects with type 2 diabetes. The serum level of cystatin C showed an AUC of 0.906 (95% CI, 0.865-0.947) with a cutoff value of 1.06 (sensitivity, 81.0%; specificity, 87.1%). Also, the urine level of cystatin C supported the diagnostic profile, showing an AUC of 0.807 (95% CI, 0.741-0.873) with a cutoff value of 0.1 (sensitivity, 70.9%; specificity, 86.3%) (Fig. 2).
Predictive factors for eGFR < 60 mL/min/1.73 m2 in normoalbuminuric patients with diabetes
We performed logistic regression analysis with ACR, CRP, glucose, low-density lipoprotein, triglyceride, high-density lipoprotein, and the cystatin C levels of serum and urine. In normoalbuminuric patients, eGFR < 60 mL/min/1.73 m2 by the MDRD equation was related to normal cystatin C levels of serum and urine by the cutoff value that was calculated from the ROC curve. When we used the EPI-equation, the factors which we put in logistic regression were ACR, CRP, glucose, low-density lipoprotein, triglyceride, high-density lipoprotein and the urine level of cystatin C. eGFR < 60 mL/min/1.73 m2 was independently related to the lower level of high-density lipoprotein (Table 3).
DISCUSSION
In this study, we aimed at evaluating the cystatin C levels of serum and urine in a small cohort of patients with type 2 diabetes by categorizing them into 3 groups depending on their different degrees of kidney damage (normalbuminuria, microalbuminuria and diabetic nephropathy). In normoalbuminuric patients, the cystatin C levels of serum and urine were significantly increased in patients with GFR ≤ 60 mL/min/1.73 m2 than those with GFR > 60 mL/min/1.73 m2. It was thought that this increment was probably due to the tubular phase before glomerular manifestation. This suggests that the cystatin C levels of serum and urine are related to subclinical tubular impairment and can be an earlier measurable markers of renal involvement before onset of albuminuria. In these patients, the cystatin C levels of serum and urine were independent factors to predict eGFR < 60 mL/min/1.73 m2 estimated by the MDRD equation. This finding indicated that the cystatin C could be an index reflecting renal tubular epithelial cells. With the EPI equation, the decreased level of high-density lipoprotein was the only independent factor to predict eGFR < 60 mL/min/1.73 m2. This result is consistent with those of previous studies demonstrating that lipid metabolism may participate in the development of glomerular and tubular alterations, leading to nephron destruction. Our results suggest that dyslipidemia can be a risk factor for kidney damage in normoalubminuric diabetic patients. Further studies are needed to confirm these results.
Our study showed that serum cystatin C was associated with CRP, ACR and eGFR, whereas urine cystatin C was associated with TG, age, eGFR and ACR in the stepwise multiple regression analysis. A recent study has suggested the relationship between cystatin C and factors such as old age, male, overweight, CRP (12), and inflammation (13). Our results are consistent with those studies.
The routine classical evaluation of diabetic nephropathy includes appearance of microalbuminuria, decreased creatinine clearance and increased serum creatinine (14). But, it has been reported that a decline in the renal function of patients with diabetes was not always accompanied by an increased ACR (15, 16). About 20%-30% of patients with type 2 diabetes, accompanied by renal insufficiency, showed normoalbuminuria (15-20). To overcome these limitations, many clinicians additionally used creatinine in evaluating such patients. However, serum creatinine also depends on creatinine production, extrarenal elimination and tubular handling (21). Moreover, tubular involvement may precede glomerular involvement because several tubular proteins and enzymes are detectable even before the appearance of microalbuminuria and a rise in serum creatinine (22, 23). Therefore, other biomarkers for estimation of renal function have been searched for and one of them was cystatin C (24). Our study results confirmed that cystain C could be one of the additional tubular factors which represent kidney state of diabetic patients.
This study has some limitations. First, owing to the retrospective cross sectional design, it was difficult to clarify the causal relationship between the risk factors and the natural course of normoalbuminuric renal insufficiency. Moreover, the patients with normoalbuinuria and eGFR < 60 mL/min/1.73 m2 might need more evaluation such as kidney biopsy to diagnose diabetic nephropathy. Second, eGFR, estimated by the MDRD or EPI-equation, did not appear to reflect actual kidney function. So, we could not conclude that which factor is more accurate or useful. Third, the subjected patients were not asked to discontinue their medications, such as antihypertensive medications. Therefore, albuminuria might be underestimated in these patients. Nevertheless, this study has some strength. We evaluated the levels of cystatin C in both serum and urine at the same time. In addition, this study demonstrated clearly that the cystatin C levels of serum and urine were increased along with the level of albuminuria in diabetic patients.
In conclusion, the results of this study suggest that cystatin C measurement in urine and serum is a useful, practical, non-invasive tool for the evaluation of renal involvement in the course of diabetes, especially in normoalbuminuric patients. Further investigations with a larger sample size and a prospective design are required to confirm the potential application of cystatin C as a useful biomarker for the early detection of diabetic nephropathy.



 XML Download
XML Download