

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Many thyroid diseases are significantly correlated with atherosclerotic cardiovascular disease (1). The thyroid hormone's regulation of lipid metabolism may represent a cause of coronary heart disease. Dyslipidemia in hypothyroidism is associated with an increased risk for cardiovascular disease (CVD); in some cases, subclinical hypothyroidism (SCH), characterized by normal free thyroxin (FT4) and elevated thyrotrophin (TSH) (2-4). Most cardiovascular events occur in subjects with normal thyroid function and the question of whether an association of TSH with cardiovascular disease exists in the euthyroid range is also important. The known associations of overt and subclinical hypothyroidism with hyperlipidemia and dyslipidemia may be extended into the normal range of thyroid function. The association of high normal TSH levels with the many cardiovascular risk factors that cluster within the insulin resistance syndrome (5-7) may be an explanation. Evidence from two studies suggests that TSH within the reference range may be positively associated with total serum cholesterol (8) and low-density lipoprotein cholesterol (LDL-C) (9), and be negatively associated with high-density lipoprotein cholesterol (HDL-C) (9). It was shown that total cholesterol (TC) and LDL-C were reduced after thyroxine treatment in individuals with TSH in the upper reference range (10). It was also demonstrated in euthyroid adults that the correlation between serum TSH and lipids appears to be influenced by insulin resistance (9). Therefore, those with an elevated amount of serum TSH and an insulin resistance are at a greater risk for dyslipidemia (11). The relationship between TSH and lipids remains controversial in subclinical hypothyroid and euthyroid subjects. We investigated whether there is a significant relationship between the levels of TSH and serum lipids; we also investigated whether the relationship may be influenced by insulin resistance or body mass index in a general population. Furthermore, we investigated the relationship of TSH and lipids in the overweight and normal weight population as well as in men and women (which was different from previous studies).
MATERIALS AND METHODS
Study subjects
Epidemiological studies on diabetes and thyroid disease were performed by the Institute of Endocrinology of China Medical University in Dadong community, Shenyang City, in 2007 (12). The database used for this study consisted of a random sample of 1,534 people between the ages of 18 and 85 yr, whose age brackets of 18-29, 30-39, 40-49, 50-59, 60-69, and 70-85 yr made up, 15.1%, 23.6%, 26.0%, 19.9%, 11.1%, and 4.4% of the total population in the community respectively.
Subjects with a history of a previous thyroid disorder, or who took thyroid hormones or antithyroid drugs, were excluded to avoid the effects of the drug. In addition, the following subjects were excluded: 1) subjects taking medication affecting thyroid function (oral contraceptives, estrogen, and glucocorticoid or anti-epileptic drugs), 2) subjects with known dyslipidemia and taking lipid-lowering medicine, 3) subjects with hyperthyroidism or hypothyroidism, and 4) subjects treated with insulin (to ensure the accurate homeostasis model assessment index for insulin resistance [HOMA-IR]). Subjects with unavailable personal data or those who known to have other kinds of diseases such as euthyroid sick syndrome and subacute thyroiditis were also excluded from this study. Finally, 1,350 subjects were included, of which 110 subjects were SCH and 1,240 were euthyroid. A total of 847 subjects (62.7%) was female.
Methods
The participants were asked to complete a questionnaire that included demographic data, smoking and alcohol history. They were asked if they ever had thyroid disease, diabetes mellitus, hypertension, dyslipidemia, or obesity. Information on treatment and family medical history was also collected. The survey was conducted between 7 a.m. and 12 p.m.. Body weight, height, waist, and hip circumference were measured. The body mass index (BMI, kg/m2) and waist to hip ratio (WHR) were calculated. Blood samples were obtained from the cubital vein after overnight fasting. After the centrifugation of blood for 30 min, the plasma aliquots were used to assay TC, triglyceride (TG), HDL-C, and blood glucose (BG) within 6 hr or were transported to the laboratory and kept at -70℃ until assayed for thyroid function and insulin.
Serum TSH and free thyroxine (FT4) were assessed using a chemiluminescent immunoassay (IMMULITE1000 Autoanalyzer, DPC, USA). Serum lipids were analyzed with an Olympus Au400 Autoanalyzer (Olympus, Tokyo, Japan), applying reagents from the No. 1 Pharmaceutical Factory of Japan. TC was measured with a cholesterol oxidase method and the TG was measured with a glycerophosphate oxidase method. HDL-C was analyzed with a selective screening method. LDL-C was calculated using the Friedewald formula: LDL-C=TC-HDL-C-TG/2.2 (mM/L). Plasma glucose was measured with a hexokinase endpoint method. Plasma insulin concentrations were measured with an immunoradiometric assay (Research Institute of North Biotechnology, Beijing, China). The homeostasis model assessment (HOMA) index for insulin resistance (HOMA-IR) was calculated as fasting insulin (mIU/L) times fasting blood glucose (mM/L, FBG) divided by 22.5.
The normal reference range of TSH is 0.3-4.8 mIU/L. FT4 (normal reference range, 10.3-24.5 pM/L) and FT3 (normal reference range, 2.3-6.3 pM/L) were measured when TSH was not in the normal reference range. Diagnostic Criteria: hyperthyroidism was TSH < 0.3 mIU/L, FT3 > 6.3 and/or FT4 > 24.5 pM/L. The criteria of subclinical hyperthyroidism was TSH < 0.3 mIU/L, FT3 and FT4 within the reference range. The criteria of hypothyroidism was TSH > 4.8 mIU/L, and FT4 < 10.3 pM/L. The criteria of SCH was TSH > 4.8 mIU/L, and FT4 within the reference range. Euthyroidism was defined when TSH was 0.3-4.8 mIU/L and FT4 was 10.3-24.5 pM/L.
Statistical analyses
SPSS 15.0 (SPSS, Inc., Chicago, IL, USA) and Excel (Microsoft Corp., Redmond, WA, USA) were used for data analysis. Data was expressed as mean ± SD for data with a normal distribution. Statistical comparisons were performed by means of independent-samples t tests or analysis of covariance to be adjusted by age, sex, and other influential factors. Pearson's correlation analysis and multiple linear regression models were performed for associations of thyroid function with serum lipid concentrations, glucose, and HOMA-IR. TG, TSH, and HOMA-IR values were logarithmically transformed for statistical analyses. P < 0.05 was considered statistically significant.
RESULTS
Comparison of lipid profiles of the SCH and euthyroid population
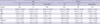
The baseline characteristics of 1,350 participants are shown in Table 1. Women with SCH had significantly lower HDL-C than those who were euthyroid. The differences remained significant after adjustment for age, sex, and BMI (Table 2). However, the HDL-C was not different between SCH and euthyroid men. Mean levels of TC, TG, and LDL-C were not different in both female and male subjects with SCH and euthyroid. Table 3 shows the comparison of TC, TG, HDL-C, and LDL-C levels according to categories of TSH within the reference range. In either men or women, there were no significant differences among the groups after adjustment for age, sex, and BMI.
Comparison of TSH by lipid profiles categories in the whole and euthyroid population
In the whole population, TC, TG, and LDL-C subclasses were each categorized as normal, high normal, and high according to the treatment guidelines of dyslipidemia for adults in China in 2007; and HDL-C subclasses were categorized as low, normal, and high. The mean TSH levels were higher in subjects in the dyslipidemia group than subjects in the normal group (results not shown). The differences were significant in high LDL-C subclasses in overweight (BMI 24.0 kg/m2 or higher according to the treatment guidelines of overweight and obesity for adults in China) individuals after adjustment for age, sex, and BMI (Fig. 1).
The mean TSH levels were significantly higher in high TC (3.76 ± 2.17 mIU/L vs 2.84 ± 2.45 mIU/L, P = 0.010) and high LDL-C (3.76 ± 2.23 mIU/L vs 2.80 ± 2.42 mIU/L, P = 0.022) subclasses in overweight women. There were no significant differences in men or overweight men (results not shown).
In 1,240 subjects with normal TSH levels (0.3-4.8 mIU/L), the mean TSH levels were significantly greater in high TC (2.40 ± 0.96 mIU/L vs 2.21 ± 1.10 mIU/L, P = 0.016) and in high LDL-C (2.44 ± 0.95 mIU/L vs 2.17 ± 1.10 mIU/L, P = 0.035) subclasses in overweight women.
Correlation analysis between TSH and lipid profiles in the whole and euthyroid population
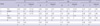
There were significant correlations of lipid profiles with age, gender, BMI and WHR in all euthyroid and SCH subjects when analysed by Pearson's correlation analysis. The TSH was associated positively with serum TG and negatively with serum HDL-C in women (Table 4). There were no significant correlations of TSH with TC, TG, HDL-C, and LDL-C in men.
Multiple linear regression models were used to determine associations of TSH with TC, TG, HDL-C, and LDL-C and to determine whether the associations were either dependent on or modified by HOMA-IR values. In the whole population, TSH was significantly and positively associated with TG, independently of the HOMA-IR value (Table 5) and was not associated with HDL-C after adjustment for age, sex, and BMI. In the overweight population, TSH was positively associated with TC (r = 0.078, P = 0.044). And the associations remained significant (β = 0.080, P = 0.039) even after adjustment for age, sex, and BMI independent of HOMA-IR value. TSH was positively associated with TC (β = 0.118, P = 0.017) and LDL-C (β = 0.118, P = 0.021) after adjustment for age, sex, and BMI in overweight women; in addition, it was not associated with TC, TG, HDL-C, and LDL-C in normal weight women, overweight and normal weight men.
In all of the euthyroid population, there were no significant correlations between TSH and serum TC, TG, HDL-C, and LDL-C. However, TSH was positively associated with TC after adjustment for age, sex, and BMI in the overweight population (β = 0.079, P = 0.050) or in overweight women (β = 0.117, P = 0.031) and the associations were not modified by the HOMA-IR values (results not shown). At the same time, TSH was not associated with TC, TG, HDL-C, and LDL-C in normal weight women and overweight and normal weight men.
DISCUSSION
The level of lipid profiles is influenced by many factors. Present research has shown that thyroid hormones change the lipid profiles. Thyroid hormones may stimulate hydroxymethylglutaryl coenzyme A (HMG CoA), the key enzyme of cholesterol biosynthesis, and induce an increased synthesis of cholesterol. Additionally, the LDL-C receptor gene contains a thyroid hormone responsive element (TRE) that could allow triiodothyronine (T3) to modulate the gene expression of the LDL-C receptor and result in an increase of LDL-C receptor synthesis (13, 14). Patients with hypothyroidism had higher baseline serum levels of TC, TG, and LDL-C and lower baseline serum levels of HDL-C. Thyroid hormones and their function are low in target tissue in SCH, and researchers conjectured that SCH influences lipid profiles by the above-mentioned mechanism.
Althaus et al. (15) reported that in subjects with SCH LDL-C levels were significant increased and HDL-C levels were decreased when compared to euthyroid subjects, after adjustment for age, sex, and BMI. The report (15) provided a possible explanation for the higher prevalence of coronary heart disease reported in SCH. The Colorado thyroid disease prevalence study (16) showed that TC and LDL-C in SCH were significantly higher than in euthyroidism; but TG and HDL-C were not significantly different. This finding was consistent with that of the studies by Efstathiadou et al. (17) in which patients with SCH had significantly higher levels of TC and LDL-C compared with controls, whereas levels of TG and HDL-C were similar in the two groups. Another study (18), however, showed that HDL-C and TG levels were similar between SCH patients and control groups. Although TC and LDL-C levels were higher in patients with SCH than in controls, the difference were not statistically significant. In this cross-sectional study of 1,350 subjects, serum concentrations of HDL-C in SCH are significantly lower than in euthyroidism; in addition, TC, TG and LDL-C were not different between the two groups after adjustment for age, sex and BMI, which was not completely consistent with previous studies.
Several factors may affect the results of the present study including age, sex, BMI, HOMA-IR, and the numbers of subjects. The numbers of previous studies were small except for the Colorado Thyroid Disease Prevalence Study. In addition, we removed the effects of age, sex, and BMI. We found that the relationship of TSH and lipids level were different in the overweight and normal weight populations, along with those in men and women.
The present data provides evidence that serum TSH has effects on serum lipid parameters in the whole population. TSH was associated positively with serum TG and negatively with serum HDL-C in women. In the whole population, TSH remained significantly and positively associated with TG after adjustment for age, sex, and BMI, independent of the HOMA-IR value. TSH was positively associated with TC in the overweight population and positively associated with TC and LDL-C in overweight women. The combination of serum TSH, sex, and BMI has important effects on serum lipid parameters.
This was suitable to the euthyroid population, that is, TSH level was associated with abnormality of TC and LDL-C in overweight women. In this study of 1,240 subjects with normal TSH levels (0.3-4.8 mIU/L), the mean TSH levels were significantly higher in high TC and high LDL-C subclasses in overweight women. TSH was positively associated with TC after adjustment for age, sex, and BMI in the overweight population or in overweight women and the associations were not modified by the HOMA-IR values. A health adult study (n = 47) (19) found that there were significant positive associations of TSH with LDL-C and TC with an inverse association with HDL-C independent of insulin sensitivity that was assessed with the hyperinsulinemic euglycemic clamp technique. In 117 diabetic women (11), the correlation between serum TSH and lipids appears to be influenced by insulin resistance; therefore, those with an elevated amount of serum TSH and an insulin resistance are at a greater risk for dyslipidemia. In 1,581 euthyroid adults, Roos et al. (19) demonstrated an association between serum TSH and TG. However, there was no relationship with other components of lipids after adjustment for age, sex, and insulin resistance. In euthyroidism (20), subjects with a TSH in the upper normal range (2.5 to 4.5 mIU/L) were more obese, had higher TG, and had an increased likeliness for metabolic syndrome. Therefore, a TSH < 2.5 mIU/L is associated with a favorable metabolic profile. Another study (21) showed an association between TSH and some components specific of the metabolic syndrome in euthyroid women. In this study, we could not find that the association of TSH with TC, TG, HDL-C, and LDL-C were influenced by insulin resistance. The conflicting conclusions maybe due to the influencing factors of age, sex, BMI, HOMA-IR, and the numbers of subjects.
In conclusion, serum TSH is correlated with dyslipidemia in subclinical hypothyroid and euthyroid subjects and the correlation was independent of insulin sensitivity.




 XML Download
XML Download