

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Interferon-alpha (IFN-α), which is the main therapeutic agent used for chronic hepatitis C virus (HCV) infection, is associated with side effects such as flu-like symptoms, hematologic abnormalities and thyroid disease. Prospective studies have shown that up to 40% of patients with HCV infection develop thyroid antibodies during IFN-α therapy (1), and around 15% develop thyroid disease (2). According to Tomer et al. (3), interferon-induced thyroiditis (IIT) can be classified as either autoimmune or non-autoimmune. Autoimmune IIT includes the de novo production of thyroid autoantibody without clinical disease, Hashimoto's thyroiditis, and Graves' disease, while non-autoimmune IIT presents as destructive thyroiditis or non-autoimmune hypothyroidism (3).
The development of thyrotoxicosis during IFN-α treatment may be due to silent destructive thyroiditis or Graves' disease. The development of Graves' disease is a less common side effect of IFN-α therapy than is destructive thyroiditis. Moreover, destructive thyroiditis followed by Graves' disease associated with IFN-α therapy occurs very rarely. Only four cases of destructive thyroiditis followed by Graves' disease asso ciated with IFN-α treatment have been reported in the literature (4, 5). Herein, we report a recent case of pegylated IFN-α (pegIFN-α)-induced destructive thyroiditis followed by transient Graves' disease in a patient with HCV infection.
CASE DESCRIPTION
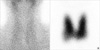
A 31-yr-old woman with hepatitis C-associated chronic active hepatitis proven on liver biopsy received pegIFN-α (Schering-Plough, Korea) 2b 100 µg weekly and ribavirin 800 mg daily from June 2009 to May 2010. Prior to pegIFN-α therapy, laboratory testing revealed normal concentrations of total T3 at 2.25 nM/L (normal range: 1.1 to 2.9 nM/L), TSH at 1.011 mU/L (normal range: 0.35 to 5.50 mU/L), and free T4 at 15.18 pM/L (normal: 9 to 26 pM/L), in addition to negative titers of antimicrosomal antibody (MSAb) at 18 U/mL (negative < 60 U/mL) and antithyroglobulin antibody (TGAb) at 26.7 U/mL (negative < 60 U/mL). Within two months of pegIFN-α therapy initiation she experienced fever, chills, headaches and dizziness. Seven months into therapy (January 2010), the patient developed mild tremors and palpitation however she had no fever or pain. There was no tenderness and palpable nodule at physical examination. She has no personal and family history of thyroid dysfunction and no specific medication history. She also had not received any test that could interfere with the thyroid scan uptake. Results of repeated laboratory tests indicated elevated total T3 at 4.26 nM/L, suppressed TSH at 0.009 mU/L, normal total T4 at 148.005 nM/L (normal: 64 to 154 nM/L), and negative titers of MSAb at 27.1 U/mL and TGAb at 31.1 U/mL. Thyrotropin-binding inhibitory immunoglobulin (TBII) was also negative at 2.6 U/L (normal range: 0 to 10 U/L). Tc-99m scintigraphy showed nonvisualization of both thyroid lobes (Fig. 1A). Based on these findings, we diagnosed the patient with interferon-induced destructive thyroiditis and prescribed propranolol 20 mg/d for one month.
Two months later (March 2010), a follow-up thyroid function test demonstrated further decline in total T3 at 3.353 nM/L, TSH at 0.013 mU/L and total T4 at 128.7 nM/L. She continued pegIFN-α therapy for an additional four months, for a total treatment duration of 12 months. Two months after the end of therapy (July 2010), she complained of hand tremors, fatigability, and 3 kg of weight loss. Laboratory tests revealed a total T3 of 12.288 nM/L, TSH of 0.004 mU/L, free T4 of 79.92 pM/L, and a TBII titer of 13.0 U/L. Tc-99m scintigraphy showed diffusely increased uptake throughout the thyroid (Fig. 1B). In thyroid ultrasonography both thyroid glands were diffusely enlarged with increased vascularities and had heterogeneous echogenicities (Fig. 2). The diagnosis of Graves' disease was made, and the patient started treatment with methimazole and propranolol. After nine months of antithyroid drug therapy (April 2011), her thyroid function tests showed normalized total T3 at 2.095 nM/L, TSH at 0.009 mU/L, free T4 at 21.36 pM/L, MSAb at 40.9 U/mL and TBII at 3.4 U/L. However, her TGAb titer was weakly positive at 63.9 U/mL.
DISCUSSION
IFN-α is an immunoregulatory cytokine that is currently used as a therapeutic agent for chronic HCV infection. Almost all patients who receive IFN-α therapy experience side effects. The most common adverse effects of IFN-α are muscle aches and fatigue, but more difficult to manage are the psychological side effects such as depression, anxiety, irritability, sleep disturbance, and difficulty concentrating (6). Our patient also experienced fever, chills, headaches and dizziness during treatment.
The association between interferon and thyroid disease was reported as early as 1985 (7). Since then, numerous studies have reported a high incidence of thyroid abnormalities in patients treated with interferon (8, 9). For many years it was assumed that side effects associated with IFN-α therapy were due to immune dysregulation. However, while immune mechanisms must play a role in the development of IIT, the predilection to the thyroid and the non-autoimmune manifestations of IIT suggest that direct effects of IFN-α on the thyroid play a major role in the etiology of IIT (10).
The most common clinical manifestation of IIT is Hashimoto's thyroiditis. Hashimoto's thyroiditis is most likely to occur during the course of treatment and has been reported in 45%-60% of patients with pre-existing thyroid autoantibodies (TAbs) compared to 3%-5% of those with no circulating thyroid antibodies prior to interferon treatment (11). Therefore, TAbs levels should be assessed prior to the initiation of IFN therapy. Our case had a negative TAbs titer prior to IFN therapy.
TAbs can develop de novo during IFN therapy or their levels can increase during IFN therapy. The majority of individuals who develop de novo TAbs due to IFN-α therapy remain TAbs-positive after treatment is completed. The incidence of de novo TAbs in interferon-treated HCV patients ranges from 10% to 40% (1, 2, 12), and TAbs develop more frequently in women treated with IFN-α than in men. Our case demonstrated de novo production of TGAb after IFN-α therapy completion. Her TGAb titer progressively increased from 26.7 U/mL to 31.1 U/mL during IFN-α therapy and remained weakly positive at 63.9 U/mL after the treatment period. The TGAb titer associated with IFN-α therapy seems to increase over time.
Classical destructive thyroiditis initially presents as transient thyrotoxicosis with decreased radionuclide uptake, which develops in three phases, followed inconsistently by a hypothyroid phase that eventually resolves spontaneously within several weeks to months. More than 50% of IIT patients with thyrotoxicosis have destructive thyroiditis. Graves' disease is characterized by overt hyperthyroidism with the presence of thyroid stimulating hormone receptor antibody (TSHRAb) and/or diffusely increased radioactive iodine uptake. IFN-α-induced Graves' disease is less common than is destructive thyroiditis, affecting 1%-2% of patients during IFN-α therapy and can manifest following INF-α therapy completion (13, 14). Typically, IFN-α-induced Graves' disease patients present with symptomatic thyrotoxicosis and do not go into remission upon completion or cessation of IFN-α therapy. In our patient, Graves' disease developed two months after IFN-α therapy completion. Her free T4 concentration was normalized after one month of antithyroid drug treatment; however, her TSH level remained suppressed after nine months of antithyroid drug therapy.
Destructive thyroiditis developed in our case after seven months of IFN-α therapy, and Graves' disease was diagnosed after treatment completion. Our case is similar to only one previously reported case. In 1995, Koizemi et al. (4) described a woman who, after three months of IFN-α therapy, successively developed transitory thyrotoxicosis, followed three months later by recurrent hyperthyroidism and the development of high TSHRAb titers. In this case, thyroid peroxidase antibody (TPOAb), TGAb, and TSHRAb titers were elevated at the time of IFN-α therapy cessation, and symptoms of Graves' disease developed four months later. Neither our case nor that reported by Koizemi and colleagues exhibited a hypothyroid phase. However, Bohbot et al. (5) reported three patients with classical destructive thyroiditis followed by Graves' disease manifesting during IFN-α therapy. In those cases, the time to the appearance of the destructive hyperthyroidism phase was 4-6 months, with the Graves' disease phase arising at 8-11 months. These intervals are slightly shorter than that observed in our case.
It is unclear how IFN-α induces Graves' disease, but the underlying mechanism is thought to be causally related to autoimmunity. The majority of patients have thyroid stimulating antibody. Some cases of transient thyrotoxicosis followed by Graves' hyperthyroidism not associated with IFN-α therapy have been reported (15-17). In those cases, destruction of thyroid tissues and release of autoantigens could have resulted in altered immunotolerance, and the subsequent production of thyroid stimulating antibody may have caused hyperthyroidism.
IFN-α can induce both autoimmune and non-autoimmune thyroiditis. However, we observed a rare side effect of IFN-α therapy as IFN-α-induced destructive thyroiditis followed by transient Graves' disease in a patient with HCV infection.

 XML Download
XML Download