

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spirometric reference values, derived from normal healthy nonsmokers, are widely used in clinical surveillance and epidemiological study to determine impaired lung function and assess the effect of environmental exposure (1, 2). Having local and native spirometric prediction equation will enhance the reliability of the evaluation of lung function (3). Results of the 2000 China Census revealed that there were 1,923,842 Korean Chinese in China, who live mostly (92.27%) in the country's three northeast provinces (4). Despite the sizeable number of Korean Chinese population, no spirometric data are available at present for them.
The project of Enlarged Population Investigation of Human Physiological Constant Database of China provides an ideal population to generate spirometric prediction equation of children and adolescents of Korean Chinese in China, of which the participants were a well-characterized group of generally healthy individuals having undergone high-quality anthropometric and spirometric measurements. As a part of Enlarged Population Investigation of Human Physiological Constant Database of China, we performed spirometry in a sample of children and adolescents of Korean Chinese to derive spirometric reference equations for them and to compare the equations with those from other populations.
MATERIALS AND METHODS
Subjects
Koreans, one of the main minorities of multiethnic China, live mostly (92.27%) in the country's three northeast provinces, and Heilongjiang being one of them (4). To perform spriometric tests during August to October, 2008, Korean Chinese children and adolescents, 8-18 yr of age, were drawn from two Korean nationality schools of Heilongjiang province- one in Harbin city, the other in Hailin city.
Clinical evaluation was based on a combination of questionnaire responses on various respiratory problems or related diagnoses and smoking status, a physical examination and 12-lead resting electrocardiography (ECG). The exclusion criteria were: any personal history of smoking; common cold within the last 4 week; history of chest injuries; respiratory disease (self-reported or medical doctor-diagnosed asthma, pulmonary tuberculosis, pneumonia, frequent bronchitis, chronic bronchitis); hypertension; respiratory symptoms during the last 12 months (chronic cough, wheezing or phlegm); clinically relevant alterations of the physical examination of the heart, lungs and chest wall; ECG abnormalities.
Measurements
Age was recorded to the nearest birthday. Standing height was measured to the nearest 0.1 cm without shoes. Spirometry was recorded with a portable spirometer (MasterLab 5.10; Jaeger, Wurtzburg, Germany). The system was calibrated with a 1-L syringe each morning and recalibrated at least every 2 hr. Integrated volumes are body temperature, ambient pressure, and saturated with water vapor (BPTS) corrected. Spirometry was conducted in accordance with American Thoracic Society (ATS) guidelines to ensure quality. (5) All measurements were carried out by an experienced research fellow and a technician. For Korean-speaking subjects, an interpreter was provided. Tests were performed with subjects in a sitting position. Nose clips were not used in this study, but nose breathing during testing was avoided by manual occlusion. Children were instructed on the technique of the maneuvers first in small groups and then the instructions were reinforced to each child individually before the test. At least three acceptable trials were required by each child in which the two largest forced vital capacity (FVC) volumes as well as the two largest forced expiratory volume in one second (FEV1) had to be reproducible within 5% of each other. The curve with the largest FVC and FEV1 was selected. Peak expiratory flow (PEF) and maximum mid-expiratory flow, (MMEF) were automatically determined by the spirometer. All tests were performed between 8:00 and 13:00.
Statistical analysis
Statistical analyses were performed using Statistical Package for Social Science (SPSS Inc., Chicago, IL, USA), version 12.0 for Windows. The data for height, age and spirometric parameters were expressed as mean ± SD. Multiple linear regression analysis was applied to observed lung function values as function of height, age and their transformation including age2, age3, log10 (age), height2, log10 (height). The effect of logarithmic and square root transformations of pulmonary function parameters prior to modeling was also examined. The form of the model and choice of independent variables were based on a combination of statistical significance (P < 0.05), the regression coefficient of determination value (R2), and other considerations related to simplicity, ease of use. The selection of prediction equations for comparison was based on common use and inclusion of the children and adolescents with the same ages as ours. The predicted values of the present study and from other studies (6-10) were compared with the measured values using paired t-tests. The difference between measured values and predicted values was expressed in terms of mean squared difference (difference = residual value/measured value) and ranked in sequence of values.
RESULTS
A total of 582 subjects with completed questionnaires underwent clinical evaluation and were allowed to perform spirometry. Of these, 139 subjects were excluded from the reference population. The reasons for exclusion and the corresponding numbers were shown in Table 1. A total of 443 subjects (226 boys and 217 girls) were included in the final analysis.
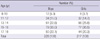
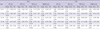
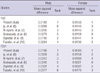
Table 2 shows the age distribution of the selected subjects for both sexes. The age range for boys was 8-18 yr (mean, 14.58 yr, and for girls was also 8-18 yr (mean 14.61 yr). Heights ranged 127 to 188 cm for boys (mean, 162.59 cm), and 127 to 171 cm for girls (mean, 156.03 cm). The height range of boys was wider than that of girls. Details of the lung function variables by age and sex are presented in Table 3.
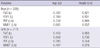
The correlation coefficients of spirometric parameters (FVC, FEV1, PEF, MMEF) with height and age are shown in Table 4. All of the spirometric parameters correlated positively with height and age significantly. The largest positive correlation was found in both sexes for FEV1 with height (r = 0.831 for boys and 0.730 for girls) and age (r = 0.789 for boys and 0.508 for girls). While the lowest correlation was observed for MMEF with both height (r = 0.652) and age (r = 0.665) in boys, and for PEF with both height ([r = 0.544] and age [r = 0.395]) in girls.
In the regression model, age and height were found to be important independent variables for all lung function parameters in both sexes. The addition of transformations did not significantly increase the explained variance, i.e. the R2 value, with more than 0.002 to 0.04. The regression equations for FVC, FEV1, PEF and MMEF based on age and standing height for two sexes are shown in Table 5.
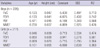
Table 6 compared the predicted values of FVC and FEV1, derived from the current authors' reference equations with other prediction equations and measured values, revealing significant differences between them. Nevertheless, there was no significant difference between all the measured values of FVC and FEV1 and predicted values of FVC and FEV1derived by reference equations of the present study.
Table 7 shows the differences between the measured values of FVC and FEV1 and the predicted values calculated from the current authors' reference equations and other prediction equations. The results showed that the predicted FVC, FEV1 values derived from equations of this work differed the least from the measured values.
DISCUSSION
The samples of our study came, as mentioned above, from two Korean nationality schools located in Harbin and Hailin respectively. The former being the capital of Heilongjiang Province, the latter a concentrated residential city for the Koreans, their Korean population was regarded as Koreans from places all over the country. Since more than 90% of Koreans in China are living in the three Northeastern Provinces; Liapning, Jilin, same and Heilongjiang, the students of the two schools, may represent average Korean Chinese children in northeast China.
Pulmonary function is known to vary by ethnicity and area, it is thus important to produce normative values relevant to the ethnic group of the local population (1-3). The present study has generated spirometric prediction equation of healthy children and adolescents of Korean Chinese in China. As with all these reference equations, they apply only to this specific group, i.e. Korean Chinese children aged 8-18 yr and with a height of 127-188 cm for the boys and 127-171 cm for the girls.
The smaller size of the 8-10 age group was determined by the higher exclusion rate of the subjects whose spirometric techniques were poor. However, as mentioned by Ip et al. (6), this did not significantly affect the curve-fitting procedure and, as a result, not the reference values functionally derived.
The predicted values of FVC and FEV1 derived from the present study were higher than values obtained by using Caucasian and other Asian equations. This finding is very different from most of other studies performed among Asians, which showed significantly less lung volumes than Caucasians (6-8, 11). The discrepancies are possibly due to several reasons, including i) differences in terms of equipments and technicians; ii) the rigorous criteria of the present study in selecting subjects, excluding not only subjects with smoking history, but also hypertension, abnormal ECG, and other; iii) regional and ethnic differences: past lung-function researches of Asians focused mostly in southeast or southwest Asia; in contrast, the present study was done in Northeast China. In addition, it is generally believed that, people from that area are both taller and stronger than their southern compatriots. Another point has to be mentioned is that there are other factors (air pollution, climate and its seasonal changes, socioeconomic differences between different groups of people, etc.) that may make it difficult to compare our results with those of other research work (12-15). In light of these factors, to evaluate the pulmonary function of children, having local and native reference equations and normative reference values are very important.
In conclusion, the present study provides the lung function predicted equations derived from a relatively large, healthy, nonsmoking young Korean Chinese population with a wide range of ages and heights. The significant differences between prediction equations obtained in current study compared with those of other studies indicate that equations based on local data should be preferred.


 XML Download
XML Download