

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Because children have a high infection rate during community outbreaks of influenza and have an important role in transmission of influenza (1, 2), sufficient vaccination coverage among children can reduce age-specific and population-level illness attack rates (3). In Korea, annual influenza immunization for all children 6 months through 59 months of age and children who are at increased risk of severe complications from influenza viral infection is included in the national immunization program. Influenza immunization for healthy children ≥ 60 months of age is recommended as an optional vaccine by the Korean Pediatric Society and the decision for administration can be made by their parents or physicians.
The influenza vaccine use in Korea has increased and the number of doses distributed/1,000 total population each year in 2003 reached the highest level in the world (4). However, all influenza vaccines were imported from manufacturers located in vaccine-producing countries. Recently Green Cross Corporation (Yongin, Republic of Korea) completed the influenza vaccine plant in Hwasun, Jeonnam Province, Korea. The first domestically developed, seasonal, trivalent inactivated influenza vaccine was available for clinical trial in 2008, and a clinical trial has been performed to examine the immunogenicity and safety of this influenza vaccine in healthy children and adolescents. There has been no publication on clinical trial of seasonal influenza vaccine in Korean children. It has been reported that this vaccine was well tolerated and induced robust immune response in both young adults and the elderly (5).
MATERIALS AND METHODS
Study design
The purpose of this study was to evaluate the immunogenicity and safety of a new trivalent inactivated split-virus influenza vaccine (GC501, Green Cross Corporation) in healthy children from 6 months to < 18 yr of age. This study was conducted as a phase III, randomized, double-blinded, active-controlled, multi-center trial at nine sites in Seoul, Gyeonggi and Gyeongnam province, the Republic of Korea. Subjects who met the entry criteria for the study were randomized in a 4:1 ratio to receive either a Green Cross influenza vaccine or active control (Fluarix®, GlaxoSmithKline Biologicals, Rixensart, Belgium). Because this study was not designed as an active control non-inferiority trial, the active control was not chosen to compare immunogenicity. The active control was used to provide information for vaccine development and production strategies in the future. The study subjects received different doses of the vaccine according to their ages. The subjects from 6 months to < 3 yr of age received 0.25 mL dose of vaccine and the subjects from 3 to < 18 yr of age received 0.5 mL dose of vaccine.
Subjects younger than 9 yr of age who had not been previously immunized against influenza received 2 doses of vaccine with one injection at day 0 and the other at day 28 (6). The vaccine was administered by intramuscular injection.
Vaccines
The study vaccine is a purified, split-virus vaccine with each dose containing 15 µg each of the three contemporary influenza hemagglutinin antigens per 0.5 mL dose (total 45 µg). The vaccine was composed of the 2008-2009 Northern Hemisphere recommended formulation: A/Brisbane/59/2007 IVR-148(H1N1), A/Uruguay/716/2007 NYMC X-175C (H3N2), and B/Florida/4/2006. The vaccine was prepared in embryonated chicken eggs with standard techniques. The control vaccine (Fluarix®) was a 0.5 mL commercial trivalent, inactivated split vaccine (Fluarix®) in pre-filled syringes containing 15 µg of each of the three contemporary influenza hemagglutinin antigens. The control vaccine contained A/Brisbane/59/2007 IVR-148 (H1N1), A/Uruguay/716/2007 NYMC X-175C (H3N2), and B/Brisbane/3/2007.
Subjects
Healthy children from 6 months to < 18 yr of age were eligible for enrollment. Exclusion criteria included hypersensitivity to any component of the vaccines (including eggs); immunosuppressive disorder; receipt of immunosuppressive or immunomodulating agents; history of Guillain-Barré syndrome; Down syndrome or cytogenetic disorder; any coagulation disorder contraindicating intramuscular injection; a current febrile illness or other acute illness; administration of gamma globulin during the previous 3 months; receipt of an influenza vaccine during the previous 6 months; and receipt of licensed inactivated or live vaccines within the preceding one month.
Safety assessment
At the first visit, parents were given a digital thermometer and a diary card containing a list of solicited adverse events and their grades. On the day of immunization day subjects were observed at the study site for a period of 30 min after vaccination to detect any immediate adverse reactions. For the next 7 days subjects or their parents recorded, in the diary card, the severity of solicited local and systemic adverse events, axillary temperature and concomitant medications taken. Subjects used a standard scale to grade adverse events (7).
The solicited local adverse events included; pain, tenderness, redness and swelling. The solicited systemic adverse events were; fever, headache, malaise, shivering, fatigue, sweating, myalgia and arthralgia. The reports of other complaints were collected during the 28 days period after vaccination. Serious adverse events were reported within 24 hr.
Immunogenicity assessment
Sampling for immunogenicity assays was performed pre-first dose (day 0) and 28 days after the last vaccination. Antibody responses were detected by means of hemagglutination-inhibition (HI) assays, according to established procedures and with use of chicken erythrocytes (8, 9), at the Korea University Guro Hospital. Titers of anti-hemagglutinin antibodies that were below the detection limit (i.e., < 1:10) were assigned a value of 1:5, and titers above 1:5,120 were assigned a value of 1:5,120.
The primary immunogenicity end points after vaccination were the proportion of subjects with seroconversion (a prevaccination titer of less than 1:10 with a post vaccination antibody titer of 1:40 or more or a prevaccination titer of 1:10 or more with a 4-fold or more increase in antibody titer) and the proportion of subjects with an antibody titer of 1:40 or more on hemagglutination-inhibition assays (seroprotection rate). The secondary immunogenicity end points after vaccination were the geometric mean titer (GMT) and geometric mean titer ratio (i.e., the ratio of the geometric mean titer after vaccination to the geometric mean titer before vaccination, GMTR) and the proportion of subjects with a prevaccination titer of less than 1:40 with a 4-fold or more increase in antibody titer.
Statistical analysis
The primary objectives of this study were to demonstrate that the lower boundary of the two-sided 95% confidence interval (CI) for the percent of subjects achieving seroconversion for HI antibody met or exceeded 40% and the lower boundary of the two-sided 95% CI for the percent of subjects achieving an HI antibody titer ≥ 1:40 met or exceeded 70% (10).
The sample size was chosen based on the power required to meet the immunogenicity endpoints. The true seroconversion rate was assumed to be at least 55%, so that with a total sample size of N = 155, the power for this comparison would exceed 96.3% for each antigen. Assuming the true seroprotection rate was at least 85%, then with a total sample size of N = 85, the power for this comparison would exceed 96.3% for each antigen. A sample size of 222 subjects in study group was designed to obtain at least 155 evaluable subjects, allowing an attrition rate up to 30%. A sample size of 58 subjects in the control group was decided as 25% of study group, allowing an attrition rate up to 30%.
The immunological and safety endpoint analyses were descriptive with calculation of two-sided 95% CI. For dichotomous variables, the 95% CI was calculated with the exact method for proportions. Geometric mean titers and 95% CI were calculated using the mean, and lower and upper limits of the 95% CI of log-transformed titers. For categorical variables, statistical summaries included counts and percentages relative to the group. All of the comparisons use the chi-square test or Fisher's exact test for contingency tables and the t-test for continuous variables. The safety population included all subjects that received a dose of influenza vaccine. All tests were two-sided with a significant level of 0.05. Statistical analyses were performed using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki and the standards of Korean Good Clinical Practice by the Korea Food and Drug Administration. The protocol and consent forms were approved by the institutional review board of each participating study site and Korea Food and Drug Administration (Biopharmaceutical Policy Division-No. 619). Informed written consent was obtained from all parents and/or participants following a detailed explanation of schedules and the contents of the study.
RESULTS
Study subjects
From September 25 to November 12, 2008, 283 subjects were enrolled. One subject dropped out after consent but before the first vaccine dose. Overall, 282 subjects who received the GC501 or control were included in the safety population (Table 1). A total of 255 subjects who received 1 or 2 doses of the GC501/control as their immunization status, and had a valid serology result were included in the immunogenicity population. Of the 255 subjects, 253 completed the study protocol (Fig. 1).
Immunogenicity
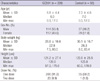
Table 2 presents the immunogenicity data on the GC501 and control vaccine groups by per protocol analysis. Seroconversion occurred in 48.5% for A/H1N1, 67.7% for A/H3N2 and 52% for B in the GC501 group. The lower boundary of the two-sided 95% CI for the seroconversion rate of each subtype exceeded 40%. For each strain, the proportion of subjects with a baseline HI titers of 1:40 or greater were similar for the GC501 and control vaccine groups. The proportion of subjects who had post-vaccination HI titers of 1:40 or greater was 90.7% for A/H1N1, 86.8% for A/H3N2 and 82.4% for B in the GC501 group. The lower boundary of the two-sided 95% CI for the seroprotection rate of each subtype exceeded 70%. Between the GC501 and control vaccine groups, the seroconversion rates and the seroprotection rates were comparable for A/H1N1 and A/H3N2. But for B strain, the seroconversion rates (P = 0.004) and the seroprotection rates (P = 0.014) were lower in the GC501 group than the control group. Geometric mean ratio was 5.6 for A/H1N1, 9.1 for A/H3N2, and 4.6 for B in the GC501 group.
Table 3 presents the seroprotection rates of the GC501 and control vaccine groups according to age by intention to treat analysis. Among subjects younger than 3 years of age in GC501 group, the proportion of subjects who achieved seroprotection was 75% (95% CI, 56.3-87.9) for the H1N1, 53.1% (95% CI, 35.0-70.5) for H3N2, and 40.6% (95% CI, 24.2-59.2) for B strain. The seroprotection rates were lower among subjects younger than 3 yr of age compared to those 3 yr of age or older in GC501 group.
Safety
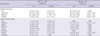
Solicited local and systemic adverse events were reported within seven days of vaccination and are shown in Table 4. Following vaccination, the solicited local adverse events were reported by 142 (62.8%) out of 226 subjects, and the most common local adverse events was tenderness, which occurred in 119 (52.7%) subjects. The solicited systemic adverse events were reported by 73 (32.3%) out of 226 subjects and the most commonly reported solicited systemic adverse event was fatigue which occurred in 43 (19.0%) subjects. Fever was reported in 5 (3.1%) out of 226 subjects and 2 of these had fever > 38.5℃. The majority of solicited adverse events were mild in intensity.
Unsolicited adverse events were reported by 53 (23.5%) out of 226 subjects during the study period. The most common events were respiratory related disorders (n = 33, 14.6%). No serious adverse events related to vaccination, or withdrawals because of adverse events were reported.
DISCUSSION
Immunization against influenza is considered to be a key public-health intervention to control both seasonal epidemics and pandemic influenza. In 2006, Global Action Plan (GAP) was developed by WHO for increasing the supply of influenza pandemic vaccines in order to reduce the anticipated gap between potential vaccine demand and supply during an influenza pandemic. They identified three main approaches: an increase in seasonal vaccine use; an increase in production capacity; and further research and development. Major progress in the development of new production capacity has been achieved by WHO support to the manufacturers of 11 developing countries. One of them is Green Cross Corporation in the Republic of Korea (11).
This study evaluated the safety and the immunogenicity of the first Korean influenza vaccine in healthy children. This influenza vaccine appeared to be safe and well tolerated. The adverse events were generally mild and consistent with previous reports for inactivated influenza vaccine in children (12, 13).
The FDA provides recommendations for clinical data to support license approvals for new seasonal inactivated influenza vaccines (10). The recommendations have been modified from guidelines by "Committee for Medicinal Products for Human Use of the European Medicines Agency" (14). For the pediatric population, the requirements are that the lower boundary of the two-sided 95% CI for the percent of subjects achieving seroconversion for HI antibody should meet or exceed 40% and the lower boundary of the two-sided 95% CI for the percent of subjects achieving an HI antibody titer ≥ 1:40 should meet or exceed 70%. Overall, the GC501 vaccine met the criteria. Previous studies reported that split-virus influenza vaccines were shown to be immunogenic for healthy children (15). The immunogenicity data of this study were consistent with previous reports that were included healthy children (15-17). However, subjects younger than 3 yr of age in GC501 group had lower antibody response to vaccine, especially for H3N2 and B antigens. In terms of the antibody responses to influenza B antigens after vaccination, the responses can be lower than responses to influenza A antigen in young children (13, 18). The numbers of subject younger than 3 yr of age were only 32 and 5 in the GC501 group and control group, respectively. The result suggest that studies evaluating efficacy of the GC501 vaccine or non-inferiority immunogenicity trials of HI antibody responses to the GC501 vaccine as compared to a licensed seasonal inactivated influenza vaccine are needed in young children.
The limitations of this study include the following. First, although it had active control group, the control group was not chosen to compare to the immunogenicity of GC501 group and the size of control group was small. Therefore, there was no useful information from the active control. Second, the study design was not stratified for the various age groups. The results showed that immunogenicity of GC501 vaccine satisfied the criteria suggested by FDA as a whole. However, immunogenicity among young children was not satisfactory, and the small number of subjects in this age group precludes any conclusion. Because the recommended doses and amounts of vaccine were different according to age, lack of stratification of age was the limitation of this study.
The results of this study indicate that GC501 vaccine has good tolerability and favorable immunogenicity in children aged 6 months to < 18 yr. An addition of one more brand of influenza vaccine might give better global accessibility of vaccine to epidemics or future pandemics.



 XML Download
XML Download