

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A patient with pneumoconiosis has to have a history of exposure to inorganic dust and certain distinctive features on simple chest radiographs (1, 2). Simple chest radiography is the principal tool of monitoring, recognizing, and classifying pneumoconiosis by the International Labour Office (ILO) classification (3, 4). With the standard analog radiographs (SARs) according to ILO guidelines, analog radiography (AR) has been widely used as the standard method for pneumoconiosis, due to relatively lower costs, good image quality, high spatial resolution, and the widely-accepted ILO classification.
We know the disadvantages of AR that include a limited exposure range, a rather high retake rate, and the inflexibility of image display and film management. Digital technology has developed an ability to offer an instant image display, a wide dynamic range, exposure latitude, and post-processing (5, 6), and previous studies showed a significant reduction of the radiation dose of more than 50% without loss of image quality compared with AR (7-9).
Digital radiography (DR) has gradually replaced AR in clinical practice, medical screening, public health surveillance, and epidemiological research as well as the recognition and classification of pneumoconiosis. Although some studies concluded that DR could replace AR in the classification of pneumoconiosis (10-13), the radiological findings of pneumoconiosis by DR may be different from those by AR because of differences in the examination methods and the image processing.
Digital images stored on Picture Archiving and Communication System (PACS) from the screening of pneumoconiosis are difficult to compare with ILO SARs, thus, a study by Franzblau et al. (12) was used to the digitalized version of the ILO SARs. In this situation, digital reference images have not been developed until now that can replace the ILO SARs. Therefore, we developed the standard digital images to be used for classifying pneumoconiosis findings on chest radiograph.
MATERIALS AND METHODS
Participants
Between July 3, 2006 and August 31, 2007, 531 retired male workers (mean age; 63.1 ± 7.9 yr, range; 42-84 yr), who were exposed to inorganic dust (mean; 19.5 ± 8.2 yr, range; 3-45 yr) participated in this study after a special examination for pneumoconiosis by DR.
Radiological examinations
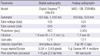
From July 3, 2006 through August 31, 2007, postero-anterior chest radiography on all participants were examined twice by DR and AR on the same day under almost identical technical conditions using a high voltage technique (120 kVp or more) in an erect position at a focus-detector distance of 180 cm. A moving grid (40 lines/cm, ratio 12:1) was used to reduce scatter (Table 1).
Digital images were captured based on the flat-panel amorphous silicon digital detector of the Philips DR system (Digital Diagnost™, The Netherlands), which has a pixel size of 143 µm (3.5 lp/mm) and a image matrix of 3,001 × 3,001 pixels (43 cm × 43 cm). The automatic exposure control (AEC) was adjusted to a 400-speed. The parameters of DR were 125 kVp, 500 mA, AEC mode, and a grid ratio of 12:1.
Analog radiographs were taken by a unit of Toshiba (MXO-15B, Tokyo, Japan), using an automatic film changer (CFC-B1000, CANON, Tokyo, Japan) combined with a wide-latitude asymmetric film-screen system (film; Fuji HR-C type, screen; Grenex HR-4 medium, size; 14 × 17 inch). The parameters of exposure were set to be similar to those of DR (124 kVp, 500 mA, and 0.005 sec); in addition, all films were developed by an automatic processor with a standard 90-sec cycle (PRO 20, DAESUNG, Seoul, Korea).
Readers and image readings
The pneumoconiosis findings on the individual digital and analog images obtained from the 531 participants were classified twice independently by four chest radiologists, with experience of more than 15 yr in the reading of pneumoconiosis, according to the ILO 2000 guidelines and SARs (2).
All images were masked for any clinical information including name, age, duration of dust exposure, and a second reading was performed about 3 months later to avoid bias. Digital images that had been transferred to a PACS system were read on monitors with a 2,048 × 2,560 pixels, and analog images were displayed on a clean standard view box in a comfortable reading room (room lighting was controllable but subdued without direct daylight).
Selection of standard digital images
Of the 531 analog images, 349 analog images (66%) were selected first in consideration of image quality: 1 = Good, 2 = Acceptable, with no technical defect likely to impair classification of the radiograph for pneumoconiosis, 3 = Acceptable, with some technical defects, but still adequate for classification purposes, 4 = Unacceptable for classification purposes, according to the ILO 2000 guidelines from reading findings, after double reading by each of the four chest radiologists on all images obtained by DR and AR using the ILO 2000 guidelines with SARs (Fig. 1) .
The pneumoconiosis findings of the 349 digital images matched with the first selected analog images were confirmed by a consensus reading of the four chest radiologists, as candidates for the standard digital images (SDIs).
From the results of the consensus reading, 120 SDIs were finally selected in consideration of the distribution of pneumoconiosis findings such as profusion, location, and shape/size of small opacity, large opacity, pleural findings, and symbols. This also included an image quality using a 4-point scale: Excellent = absence of any defects, Good = some defects in position, Fair = presence of one or both scapula(e) in lung field, Poor = not completely visible costophrenic angle. A set of 120 SDIs is included various parenchymal and pleural findings that the absence in ILO SARs (e.g. profusion 0/1, 1/0, 2/3, 3/2, 3/+, shape/size u, symbols aa, at, cn, co, cv, di, fr, kl, px, tb).
RESULTS
Image quality
The 120 SDIs were of a fair grade or more using a 4-point scale for image quality. There were 85 excellent (70.8%), 11 good (9.2%), and 24 fair (20.0%) grade images.
Parenchymal findings
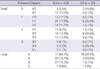
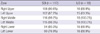
Of the 120 SDIs, 15 images had no definite pneumoconiotic findings and profusion Category 1, 2 and 3 were in 50, 40, and 15 images, respectively (Table 2). Images with large opacity were 43 (35.8%). Small opacities were distributed more frequently in the upper and middle lung than the lower lung (Table 3). In primary small opacity, p, q and r for rounded opacity were 28, 40 and 22, and s, t and u for irregular opacity were 2, 23 and 2, respectively (Table 4). In secondary small opacity, p, q and r were 16, 35 and 20, and s, t and u were 11, 28 and 7, respectively. Irrespective of primary or secondary, q and t was the most frequent in rounded and in irregular opacity, respectively.
Pleural findings
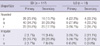
Of the 120 images, 31, 9, and 11 images showed pleural plaque (PP), diffuse pleural thickening (DPT), and costophrenic angle (CPA) obliteration, respectively (Table 5). On the 31 images, we found 46 PPs on the either one or both sides of chest wall. PPs of the chest wall were more frequent on the right side (32 vs 14), and were accompanied by calcification in 4 cases. In addition, PPs shown as in profile were more frequent than that as face-on (38 vs 8). Three images had two PPs shown as in profile and face-on on the same side and extended up to 1/4 (3 images) and from 1/4 to 1/2 (1 image) of chest wall after summation.
On the 9 images, we found 12 DPTs on the either one or both sides of the chest wall. DPTs were more frequent on the right side (8 vs 4), and accompanied by calcification in 3 cases. In addition, DPTs shown as in profile were more frequent than that as face-on (10 vs 2). Two images had two DPTs shown as in profile and face-on on the same side and extended more than 1/2 of the chest wall after summation. CPA obliteration was found more frequent on the right side (7 vs 4). Seven CPA obliterations were accompanied with diffuse pleural thickening (right 5 vs left 2). Calcification was found in 6 PPs of 4 images (chest wall 4 and diaphragm 2) and 3 DPTs of 2 images. They were more frequent on the right side (6 vs 3).
Symbols
Twenty-nine symbols are additional features related to dust exposure and other aetiologies, and use of symbols is obligatory. The symbols are: atherosclerotic aorta (aa), significant apical pleural thickening (at), coalescence of small opacities (ax), bulla (bu), cancer (ca), calcified non-pneumoconiotic nodules or nodes (cg), calcification in small pneumoconiotic opacities (cn), abnormality of cardiac size or shape (co), cor pulmonale (cp), cavity (cv), marked distortion of an intrathoracic structure (di), pleural effusion (ef), emphysema (em), eggshell calcification of hilar or mediastinal lymph nodes (es), fractured rib (fr), enlargement of non-calcified hilar or mediastinal lymph nodes (hi), honeycomb lung (ho), ill-defined diaphragm border (id), ill-defined heart border (ih), septal (Kerley) lines (kl), mesothelioma (me), plate atelectasis (pa), parenchymal bands (pb), pleural thickening of an interlobar fissure (pi), pneumothorax (px), rounded atelectasis (ra), rheumatoid pneumoconiosis (rp), tuberculosis (tb), other disease or significant abnormality (od). Instead of 15 symbols on the ILO SARs, we found 21 symbols out of 29 symbols except cp, ef, ho, id, me, pa, ra, and rp on the 120 SDIs. The ax was found most frequently in 64 images (53.3%), and bu, tb, em, pb, cg, at, and aa were in 40, 35, 21, 19, 18, 14, and 10 images, respectively. Each of hi and kl in 8, and each of es and fr in 7, each of ca and cn in 6, each of ih and pi in 5, each of di and od was found in 4 images; however, co, cv, and px were found only in one image.
DISCUSSION
Simple chest radiography has traditionally been used for the recognition of pneumoconiosis in dust-exposed workers. Currently, the ILO 2000 guidelines with 22 standard analog radiographs are used for classifying pneumoconiosis in the world.
The patient with pneumoconiosis has been increased a few each year in Korea although decline of the coal mining industry (14), and DR have being replaced instead of the AR for screening pneumoconiosis.
Since DR was introduced in the early 1980s (15), it has been well accepted in clinical practice because of easy handling, less chemical waste, less space for storage, and better latitude as well as a possible reduction of the radiation dose without a loss of image quality compared to AR in chest radiology (8, 9, 16). Previous studies demonstrated that DR can replace AR as the standard method in the diagnosis and classification of pneumoconiosis (10-13).
During the pneumoconiosis classification, the ILO requires that the patient's radiograph should be compared side-by-side to the appropriate comparison images from the ILO standard reference set that consisted of 22 analog radiographs. However, it is very uncomfortable for reader to compare patient's radiograph to the multiple reference radiographs simultaneously or in turn. In addition, a reader using DR has to compare the digitalized pneumoconiosis findings to the ILO SARs because standard digital images are not developed. However, it is impractical to use a separate view box to display the ILO SARs because it degrades the workflow and alters the perception of the pneumoconiosis findings.
First, it is improper to compare digital images with analog radiographs. Takashima et al. (11) reported that in the application of DR to the medical screening of dust-exposed workers, it is difficult to compare subject's images with the ILO SARs. It is even more difficult to read digital images on PACS compared to the ILO SARs directly. Franzblau and colleagues (12) demonstrated that the digitalized version of the ILO SARs may provide an approach for the implementation of the ILO classification for digital images; however, it could not ensure reliability and validity because pneumoconiosis findings could be different between the soft-copied and hard-copied image. Original analog images were more accurate than corresponding digitalized images (97% vs 89%) in the diagnosis of interstitial lung diseases (17). In the study reported by Mannino et al. (18) the interpretation of digitalized images for small opacities of pneumoconiosis was different from that of original analog images. In this situation, it is imperative to develop the standard digital images for the classification of pneumoconiosis instead of the ILO SARs.
We tried to ensure the validity and reliability of digital images that can be used as standard for the classification of pneumoconiosis. First, all digital images and analog radiographs were obtained according to the guidelines for chest radiography, such as high kVp (120 or more), short exposure time (below 0.03 sec), and grid ratio of above 10:1. Second, after digital images and analog radiographs were taken simultaneously from the same examinee, pneumoconiosis findings on the all images were classified twice according to the ILO guidelines and SARs by four chest radiologists with experience of more than 15 yr in the reading of pneumoconiosis findings. Third, 120 SDIs were selected to consider the distribution of pneumoconiosis findings on the corresponding analog radiographs by a consensus reading of the four chest radiologists.
Pneumoconiosis findings on a chest radiograph can be significantly affected by the image quality (2, 6), and it is very important to acquire highly qualified images. An optimal image for the classification of pneumoconiosis should reveal the fine detail of parenchymal markings, clearly demonstrate the CPA, and show vascular markings through the cardiac and subdiaphragmatic shadow. In addition, common quality faults include an under-exposure that is often associated with a tendency for the over-estimation of profusion and the over-exposure associated with the reverse tendency (3). We selected the 120 SDIs that had an image quality grade of fair or more. Therefore, they may have some defects in the examinee's position or presence of scapula(e) in lung field. However, the ILO SARs also have some technical defects such as over or under exposure, invisible costophrenic angle, and presence of scapula(e) in lung field.
Digital images can be produced from the various detector systems such as computed radiography based on the imaging plate (CR), a flat panel based on amorphous silicon (a-Si DR), a flat panel based on amorphous selenium (a-Se DR), and charge-coupled device (CCD). These systems have different basic image quality parameters to indicate the performance of the detector such as a detective quantum efficiency (DQE) and modulation transfer function (MTF) (19, 20). In our study, digital images were produced by the detector based on a-Si DR to provide more superior image quality to other detector systems and to allow the potential of reduction in radiation dose (9, 16, 20, and 21).
Our set of 120 SDIs includes all categories of small and large opacity and has variable shape and size of small opacity, whereas ILO SARs have not some subcategory which is 0/1, 1/0, 2/3, 3/2, and 3/+. Our SDIs have more pleural findings than ILO SARs, except one composite radiograph with pleural findings. In addition, they have symbols that are not in the ILO SARs (aa, at, cn, co, cv, di, fr, kl, px, and tb).
In a digitalized environment it is not problem that our SDIs have more reference images than the ILO SARs (120 vs 22), because of the easy and rapid reference from a server or compact disc after storing the SDIs. The image quality of analog radiographs may deteriorate and change the pneumoconiosis findings over time; however, the stability of SDIs does not change over an extended period of time. The 120 SDIs are encoded in Digital Imaging and Communication in Medicine (DICOM) files to maximize the consistency of display on different workstations and to allow it to be stored within PACS. This study was performed independently with ILO.
A set of 120 SDIs have more various pneumoconiosis findings than ILO SARs and was developed from adequate methods. It can be used as the digital reference images for the recognition and classification of pneumoconiosis.


 XML Download
XML Download