

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Both the Child-Turcotte-Pugh (CTP) classification and the model for end-stage liver disease (MELD) score are used as general indicators of the severity of liver failure in patients with end-stage liver disease. Many studies have been conducted to evaluate which of the two indicators is more reliable. The studies have focused on the indicators' reliability for establishing priority for liver transplantations (1, 2), evaluating health-related quality of life and predicting mortality (3-5), predicting survival after liver transplantation or hepatic resection (1, 6-9), and predicting prognoses regarding other liver diseases, such as cirrhosis, carcinoma, and hepatitis (10-13).
Studies have shown that cytokine concentrations in patients undergoing liver transplantations can be used to predict the graft prognosis (14-17). This suggests that the CTP classification or the MELD score may be useful in assessing the degree of systemic inflammatory reaction in liver transplantation patients by measuring cytokine concentrations. However, comparison of the ability to predict the severity of the systemic inflammatory response by immunological reaction between the CTP classification and the MELD score has not been prospectively evaluated.
In this study, we investigated the usefulness of the CTP classification and the MELD score in assessing the degree of systemic inflammatory reaction in patients undergoing liver transplantation and compared the reliability of the two indicators.
MATERIALS AND METHODS
This prospective study was conducted in a cohort of living-donor liver transplantation (LDLT) donors and recipients with liver cirrhosis between January and December 2008. Patients with a history of abdominal surgery, those with an unstable preoperative cardiovascular status, those with severe hypoxemia due to acute respiratory distress syndrome (ARDS) or hepatopulmonary syndrome (HPS), those who had evidence of infection other than viral hepatitis, those who required intraoperative veno-veno bypass or hemodialysis and minors (less than 18 yr old) were excluded. Healthy donors were allocated to a donor group, and the recipients with liver cirrhosis were assigned to a recipient group.
The CTP classification and the MELD scores of the patients in the recipient group were assessed at preoperative visits, based on the most recent laboratory data. The CTP scores were calculated using levels of prothrombin time, albumin, bilirubin, and clinical ascites and encephalopathy findings and stratified as class A (5-6), B (7-9) or C (10-15) (18). The MELD scores were assessed using three individual factors that affect the liver transplant prognosis: serum total bilirubin, serum creatinine, and the prothrombin time-international normalized ratio (PT-INR); the values were applied to a multivariate regression model (MELD Score = 9.57 × loge[creatinine mg/dL] + 3.78 × loge[bilirubin mg/dL] + 11.20 × loge[INR] + 0.643) (19).
A right lobe hepatectomy was performed on the LDLT donor patients and transplanted into the recipients. Liver allografts were preserved in University of Wisconsin solution. None of the patients received veno-veno bypass or temporary portocaval anastomosis. After general anesthesia was induced, a 20-gauge angiocatheter was inserted into the right radial artery and 10 mL of fresh blood was collected for the preoperative serum cytokine level analysis. In the recipients, additional blood samples were collected at 60-min after the start of the anhepatic stage (inferior vena cava is clamped above and below the liver, as are the hepatic artery, portal vein, and common bile duct) and at 60-min post-reperfusion. Blood samples were delivered to the laboratory in a test tube, which was preserved in an ice-filled container and centrifuged (1,300 rpm, 5 min, 4℃). The separated serum was frozen at -70℃.
The pro-inflammatory cytokines measured included tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-6; the anti-inflammatory cytokines included IL-4 and IL-10. Cytokines were quantified using commercial sandwich enzyme-linked immunoassay kits (Quantikine; R&D Systems, Minneapolis, MN, USA).
Parametric data are presented as means ± SD, and nonparametric data are presented as medians with quartiles. The SAS software (ver. 8.02; SAS, Inc., Cary, NC, USA) was used for statistical analyses. Based on data from a pilot study, the expected correlation coefficient for preoperative MELD scores and the cytokine concentrations was 0.45. A sample size of 36 patients in each group was required to achieve a power of 80% with an alpha error of 0.05. To compensate for potential dropouts, we enrolled 43 patients in each group. The Mann-Whitney rank-sum test was used to compare cytokine levels between the two groups, and the Friedman test was used to compare the intra-operative cytokine concentrations according to the CTP classification. The impact of the CTP score and the MELD score on the cytokine levels was evaluated with Spearman's rank correlation coefficient. P values < 0.05 were considered to indicate statistical significance in all analyses.
Ethics statements
The study was approved by the institutional review board of the Seoul St. Mary's Hospital (number: KCMC070T268) and registered with CRiS (identification number: KCT0000038). It complies with the standards of Declaration of Helsinki. Written informed consent was provided by each patient prior to participation in the study.
RESULTS
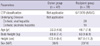
In total, 86 patients were recruited for the study but 5 were excluded based on the exclusion criteria. One patient in each group declined to participate in the study and 3 patients in the recipient group showed preoperative cardiovascular instability or severe hypoxemia, so data from 81 patients were finally analyzed. In the recipient group, 29 patients were diagnosed with cirrhotic viral hepatitis, and 10 were diagnosed with cirrhotic alcoholic hepatitis. Patient characteristics are shown in Table 1.
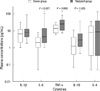
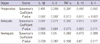
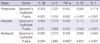
The IL-6, TNF-α, and IL-10 concentrations in the recipient group were significantly higher than those in healthy donor group patients (Fig. 1). Preoperative concentrations of cytokines, except IL-6, were higher in patients with CTP classifications indicating increased severity of liver disease. During the perioperative period, the correlation between the cytokines and the severity of liver disease diminished. However, TNF-α and IL-4 concentrations during the anhepatic stage and the IL-6 and IL-4 concentrations during the neohepatic stage (post-reperfusion) were significantly higher in patients with severe liver disease (Table 2). All of the cytokine concentrations, except IL-6, were significantly correlated with the CTP scores and the MELD scores preoperatively. The correlations diminished during the surgery, although TNF-α and IL-4 concentrations continued to be correlated with the MELD scores (Tables 3, 4).
DISCUSSION
Our results show that both the CTP classification and the MELD score, indicators of the severity of liver disease, are valid tools for predicting the severity of the systemic inflammatory reaction in patients with liver cirrhosis who underwent living-donor liver transplantation. Perioperative secretion of cytokines in patients undergoing liver transplantation is closely related to the graft prognosis. Boros et al. (14), found that IL-1, IL 6, and IL-8 concentrations in the hepatic vein at the time of reperfusion were higher in patients who suffered poor postoperative graft function, and Hassan et al. (15) reported that plasma concentrations of IL-6 and IL-10 might be useful as predictive indicators for postoperative complications in liver transplant recipients. Mueller et al. (16) also reported that several cytokines secreted during liver transplantation, including IL-2, were correlated with postoperative graft function. The proposed mechanism is excessive secretion of cytokines, promoting graft inflammation, resulting in a loss of graft function (17). Thus, it seems likely that the CTP classification or the MELD score, which are used to predict survival after liver transplantation, may also be useful in estimating the severity of the systemic inflammatory reaction, which is measured in terms of plasma cytokine concentrations. In this study, we evaluated perioperative cytokine concentrations according to the CTP classification and the MELD score of the patient and then analyzed which indicator was more closely related to cytokine concentrations. Before surgery, the concentrations of all of the cytokines measured, except IL-6, were higher in patients with more severe liver disease, as classified according to the CTP classification and the MELD score. This indicates that severity of the systemic inflammatory reaction before liver transplantation can be estimated with equal reliability using the CTP classification and the MELD score.
Both the CTP classification and the MELD score have been used to prioritize patients for orthotopic liver transplantation and to evaluate pre-transplantation health related quality of life, as well as to predict post-transplantation mortality. Although they are both used as indicators of patient prognosis, there is controversy regarding which is the more reliable indicator. The controversy stems from differences in underlying diseases, research centers, and research methods. This study shows that in both the CTP classification and the MELD scoring system, a poor prognosis was associated with higher preoperative cytokine concentrations, which suggests that both rating systems are useful for predicting the severity of the systemic inflammatory response in patients with end-stage liver disease. This result is consistent with those of Boin et al. (2), Said et al. (5), and Mishra et al. (20), who suggested that both the CTP classification system and the MELD scores were equivalent for determining the outcome of patients suffering from chronic liver disease.
The reason both the CTP classification and the MELD score are equivalent in estimating the severity of the preoperative systemic inflammatory response is that the factors constituting the CTP classification and the MELD score are closely related to the clinical and laboratory findings in patients with systemic inflammatory response syndrome (SIRS) or sepsis. Cazzaniga et al. (21) demonstrated that the prevalence and in hospital outcome of SIRS in patients with cirrhosis were correlated with high serum bilirubin levels, high PT-INR, and high serum creatinine levels, all of which are constituent factors for the MELD scores and two of which contribute to the CTP classification. Also, SIRS mediators may exacerbate the neuropsychological effects of hyperammonemia in cirrhosis (22). Additionally, bacterial translocation, the main bacterial entry route into the cirrhotic host, was significantly increased in Child C patients (31%), compared with Child B (8%) and Child A (3%) patients (23). Thus, we can conclude that the systemic inflammatory response that occurs in end-stage liver disease patients may result in a more severe preoperative CTP classification and MELD score.
During the intraoperative period, the relationship between the CTP classification or the MELD score and the cytokine levels diminished or disappeared. Cytokine level trends during surgery were different from those during the preoperative period. Although IL-4 levels were closely correlated with the CTP classification, the CTP score, and the MELD score throughout the surgery, other cytokine levels were not. TNF-α levels had a significant correlation with the MELD scores during the anhepatic and neohepatic stage, but not with the CTP score during any stage. IL-6 concentrations were closely related to the CTP classifications during the neohepatic stage, but not with the CTP or the MELD scores during any stage. Thus, it appears that the correlation of cytokine levels with the liver disease indicators varied according to the time of measurement during the surgery, not because of differences between the indicators themselves. This is supported by the fact that the CTP classification, the CTP score, and the MELD score had statistically similar correlations with the concentration of each cytokine in preoperative measurements. That is, the main factor impacting cytokine secretions during surgery is surgical stress from extensive tissue injury, clamping of great vessels, deterioration of acid-base balance, massive bleeding and transfusion, and severe hemodynamic instability.
This study had both a controlled and prospective design, and we excluded patients with a history of abdominal surgery, those with an unstable preoperative cardiopulmonary status, and those who were under veno-veno bypass or hemodialysis during surgery. Furthermore, the underlying disease caused liver failure was confined to the cirrhotic hepatitis. These allowed us to remove several important factors other than the preoperative CTP classification and MELD score that may have impacted the severity of the systemic inflammatory response.
Plasma concentrations of IL-6, TNF-α and IL-10 were significantly higher in patients with liver failure than in healthy subjects (donors), confirming the difference in the stress response between the two groups. This stress is the result of dysfunction in multiple organs, including the liver, as well as systemic inflammation. Measuring plasma cytokine levels is a way to indirectly determine the degree of inflammation and stress in a patient with liver failure. However, the difference in cytokine concentrations between healthy subjects and patients with liver failure seen in this study may not be a true reflection of disease severity, because blood samples were collected in the operating room after the induction of anesthesia. Drugs administered to induce and maintain anesthesia, the response to tracheal intubation, and a patient's preoperative anxiety could be stress factors that interfere with assessing the influence of end-stage liver disease on cytokine concentrations. Reports that anesthesia itself has an impact on the immune response support this (24-26). Nevertheless, the study showed clear differences in the cytokine concentrations between donor and recipient groups and factors associated with anesthesia should have affected both groups equally. Thus, we conclude that differences in the cytokine concentrations were a reflection of the severity of liver disease.
In conclusion, the plasma levels of cytokines in patients with liver failure increase according to the severity of liver disease, as indicated by the CTP classification and the MELD scores, but they were less correlated during the intraoperative period. The severity of the systemic inflammatory reaction prior to liver transplantation is estimated with equal reliability using the CTP classification and the MELD score. The results of this study provide another application of the CTP classification and the MELD scores.

 XML Download
XML Download