

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiovascular diseases such as coronary artery disease (CAD) and stroke are among the leading causes of death in Asian populations as well as in Western countries (1). Oxidative stress is thought to play an important role in the progression of atherosclerosis (2, 3). Several studies have implicated gamma glutamyltransferase (GGT) as a biomarker of oxidative stress and exposure to xenobiotics (4, 5). Parallel evidence from epidemiological studies suggest that higher serum GGT is associated with development of CAD risk factors, including diabetes, high blood pressure (BP) and dyslipidemia (6-9), and metabolic syndrome (6). GGT levels are related positively to novel cardiovascular risk factors such as C-reactive protein (CRP) and fibrinogen (10), and are inversely related to antioxidant levels (11). Increased GGT has been linked with mortality attributable to CAD and cerebrovascular disease (12, 13). In spite of the clinical impact these increased GGT levels have in western countries, however, it is little known the effect of GGT levels in the prediction of the CAD risk in Asian population. The Framingham Risk Score (FRS) is a mathematic model for predicting CAD during a 10-yr period that has become a widely-used clinical tool to guide the delivery of preventive medicine (14, 15).
The present study was grounded in the hypothesis that increasing serum GGT is associated with the risk of CAD, calculated using FRS modified by the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) guideline, and should be considered as a factor associated with CAD risk prediction. The aim of this study was to examine whether serum GGT levels are associated with FRS in Koreans.
MATERIALS AND METHODS
Study data
From January 2007 to May 2009, data of 42,906 Koreans aged 20-86 yr who visited the Health Promotion Center, Ajou University Hospital, Suwon, Korea, were reviewed for inclusion in the study. Medical history, demographics, anthropometric, and laboratory data were collected. Data on cigarette smoking and alcohol consumption were collected by a self-reported questionnaire. Subjects who, at the time of the survey, had smoked cigarettes regularly within the prior year were considered to be current smokers and weekly alcohol intake was calculated and then converted to weekly alcohol consumption (grams of ethanol per week) by graduated frequency method (16). Of the initial 42,906 subjects, 9,256 (21.5%) were excluded because of absent data for any component of FRS or smoking or alcohol history. We also excluded subjects (n = 1,124) with hepatobiliary disease, positive tests for antibody to hepatitis B surface antigen, antibody to hepatitis B virus core antigen or anti-hepatitis C virus, and patients (n = 1,012) taking drugs influencing liver function and statins or other lipid-lowering drugs, and subjects (n = 804) with high sensitive CRP (hs-CRP) ≥ 10.0 mg/L to preclude any possible occult inflammatory or infectious disease. Thus, a total of 30,710 healthy Korean (13,777 females, 16,933 males) were included in the final analyses.
Measurements
Serum GGT was assayed by the standard method recommended by the International Federation for Clinical Chemistry using L-γ-glutamyl-3-carboxy-4-nitroanilide as substrate with a Toshiba 200FR autoanalyzer. Hs-CRP was measured by a high-sensitivity nephelometric method (Dade Behring Marburg GMBH, Marburg, Germany). BP was measured using a standard mercury manometer with the participant in a sitting position for 5 min prior to measurement; the average of two measurements was recorded. Hypertension was defined as a systolic BP 140 mmHg or a diastolic BP 90 mmHg, or the use of antihypertensive medication. Fasting blood specimens were used for measuring lipids, glucose, and liver enzymes. Diabetes was defined by fasting blood glucose 126 mg/dL or the use of oral hypoglycemic agents or insulin. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
Statistical analyses
The distribution of GGT values and alcohol consumption were right-skewed, therefore a natural log-transformation was applied. To assess the relationship between biomarkers and the individual components of the FRS, Pearson correlation coefficients relating individual risk factor scores and the total of FRS to log-transfomed GGT levels were analyzed. The study subjects were grouped into quartiles according to the circulating levels of GGT. We examined the mean FRS according to the quartile of serum GGT concentration. ANOVA Trend analysis using polynomial contrasts was adapted to perform tests for trend. Framingham risk equations (14) were used to predict the risk of developing total coronary disease events (angina, myocardial infarction, or coronary heart disease [CHD] death) over the next 10 yr. Participants were divided into three groups (17): low risk (≤ 9% risk of developing a CHD event over the next 10 yr), intermediate risk (10%-20% risk), and high risk (> 20% risk). For analyses relating GGT to high-risk for CAD (10-yr risk ≥ 20%), we constructed adjusted logistic regression analyses that considered age/gender, age/gender + alcohol consumption + BMI, and (age/gender + alcohol consumption + BMI) + novel and conventional risk factors including hs-CRP, diabetes, low density lipoprotein (LDL) cholesterol and uric acid. Results of group data are expressed as mean ± standard deviation (SD). All statistical analyses were performed using SPSS 13.0 software (SPSS, Chicago, IL, USA). P values < 0.05 were considered statistically significant.
RESULTS
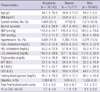
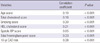
Compared with women, men presented with more CAD risk factors such as diabetes mellitus, hypertension, dyslipidemia, alcohol consumption and current smoking (Table 1). Therefore, the total Framingham point score and 10-yr CAD risk were higher in men than in women. The correlation coefficient between log-transfomed GGT levels and FRS was r = 0.38 (P < 0.001) in the study subjects (Table 2). These positive correlations were of consistent in men (r = 0.19; P < 0.001) and women (r = 0.21; P < 0.001) (data not shown). Serum GGT also was well correlated with individual risk factors. The median (range) of the first-to-fourth quartiles of GGT values was 11.17 (4-14), 18.11 (15-22), 29.67 (23-39), and 83.46 (≥ 40) IU/L, respectively. Increasing the quartile of serum GGT concentration was significantly associated with linear increasing trends in FRS (P trend < 0.001) (Fig. 1). Compared to the lowest baseline GGT category, age-gender adjusted odds ratio (OR) for FRS ≥ 20% were 3.1, 5.0, and 7.5 (P for trend < 0.001) in the other three GGT categories (Table 3). The relationship remained statistically significant after additional adjustments for alcohol consumption and BMI. Further adjustments for known CAD risk factors attenuated this relationship, but GGT remained a significant risk factor in a model that included hs-CRP, uric acid, LDL cholesterol and diabetes (Table 3).
DISCUSSION
The present data demonstrate that serum GGT levels positively correlate with the risk of CAD calculated using the FRS. The association was not confounded by alcohol or the other known CAD risk factors (LDL cholesterol, BMI, hs-CRP, uric acid and diabetes).
Although GGT has been widely utilized as a marker for alcohol consumption or liver disease (18, 19), a large number of studies suggest that GGT is not only a marker for oxidative stress (4, 20) but also a relative factor of cardiovascular disease and metabolic syndrome (6, 12, 13, 21). Increased oxidative stress and systemic inflammation are considered key factors for the progression of atherosclerosis and CAD (2, 11-13). Thus, it was hypothesized that GGT could be a marker for CAD risk prediction, regardless of alcohol consumption. Our data show that, compared to the lowest baseline GGT category, the OR of FRS ≥ 20% increased significantly with increased serum GGT levels. After adjustment for age, gender, alcohol consumption and other known CAD risk factors, the relationship between GGT and FRS ≥ 20% remained significant. The cut-off of fourth-quartile GGT levels was defined as > 40 IU/L. This value is considered an abnormal GGT level according to most medical laboratories. The observations that the OR of high-risk for CAD by GGT quartile was significantly increased within the normal reference range of GGT levels suggest that GGT could be regarded as a risk stratification marker of FRS ≥ 20%, despite the normal reference range.
What is the possible underlying mechanism to explain the observed link between serum GGT levels and CAD risk prediction? First, although the mechanisms that explain the contribution of GGT to CAD have not been fully elucidated, GGT is related to hepatic steatosis (22) and insulin resistance (23), and is a predictor of incident diabetes (24) and hypertension (25). These results suggest that there is a potential role of GGT-mediated reactions in atherogenesis. Indeed, the potential role of GGT in promoting plaque formation and evolution has been confirmed by the identification of catalytically-active GGT in coronary, cerebral and carotid plaques, colocalized with oxidized LDL and CD68+ foam cells (26). Second, GGT activities may also modulate the redox status of protein thiols at the cell surface, leading to the production of free radicals and reactive oxygen species, and LDL oxidation (27, 28). Thus, GGT is considered a factor that contributes to oxidative stress pathways in various organ systems, localizes to atheromatous plaques containing oxidized lipoprotein, and is proinflammatory, further implicating this protein in atherogenesis (29, 30). These observations may explain the finding of an association between serum GGT levels and CAD risk prediction.
This study has several strengths and limitations. One of the strengths is the large scale of the study, with subjects of both gender and all age groups. Therefore, the results can be generalized into the entire Korean population. Second, we used the categories of the estimated 10-yr CAD risk calculated by using the NCEP ATP III, which is considered the current standard for prediction of CAD risk. But, the present study was cross-sectional and we did not investigate oxidative stress markers, and thus could not examine any association of oxidative stress with serum GGT levels.
In conclusion, the present study demonstrates that serum GGT levels are associated with the estimated 10-yr CAD risk calculated by using NCEP ATP III in Korean. These significant associations in serum GGT levels even within the reference range appear to have an additional benefit in the prediction of future development of CAD. Thus, serum GGT may be helpful to predict the future risk of CAD. Further longitudinal cohort studies are needed to evaluate the predictive value of biomarkers for the risk of CAD in Koreans.


 XML Download
XML Download