

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Clostridium difficile infection (CDI) has been a common healthcare-associated infection since the first recognition as a cause of pseudomembranous colitis in 1974. Emergence of hypervirulent strains changed clinical characteristics and epidemiology of CDI in North America (1). North American pulsed-field type 1 (BI/NAP1/027) is the most common hypervirulent strain and have influenced five-fold increase in incidence and mortality of CDI (2). Nevertheless, there are few data about epidemiology including prevalence and disease course of CDI in Korea, although several retrospective clinical and microbiologic data were published (3, 4).
This is an observational study to investigate the incidence of CDI and distribution of toxigenic C. difficile strains in Korea. We also observed demographic, clinical characteristics and treatment outcome of CDI as a baseline data for further study.
MATERIALS AND METHODS
Design of study
This study was conducted at Hanyang University Hospital, a 900-bed tertiary care facility located in Seoul, Korea. From September 2008 through January 2010, all patients whose stools were tested for toxin assay A&B and C. difficile culture were included in the study. Clinical characteristics of the patients were observed prospectively, and isolates from the patients were collected for further study.
Definition
Diarrhea was defined as unformed stools more than 3 times per day on consecutive days or 6 times within 36 hr. Antibiotic-associated diarrhea (AAD) was defined when patient had diarrhea and there was no reason for diarrhea except antibiotics use (5). We diagnosed CDI when the C. difficile isolates from stool culture showed positive toxin genes (tcdA, tcdB, cdtA, or cdtB) by multiplex PCR, positive results in toxin assay A&B with commercial kit (VIDAS® C. difficile Toxin A & B; BioMerieux SA, Marcy l'Etoile, France), and/or pseudomembrane on endoscopy or histology in patients with AAD.
The CDI patient who developed diarrhea at least 72 hr after hospitalization or within the 2 months from last discharge when the patient did not reside in healthcare facilities was considered as Healthcare-associated CDI (HA-CDI). If the case did not meet the definition of HA-CDI, we considered it as community-onset CDI (CO-CDI) (6). Patients with C. difficile containing positive toxin genes in stool or positive results of toxin assay A&B but whose stool characters did not meet the criteria of diarrhea was considered as toxigenic carrier. Patients with C. difficile without toxin genes in stool were non-toxigenic carrier.
Collection of data
Age, sex, length of stay in hospital, operation history and medication history within 2 months, and underlying disease including Charlson's score were investigated as demographic and clinical data. Instillation of catheter, use and amounts of antibiotics, probiotics, proton pump inhibitor, H2 blocker, steroid, or chemotherapy, and recent operation within 2 months were studied as a risk factor of CDI (7). Amounts of antibiotics administered were expressed as the number of defined daily dose (DDD), which means the total amount of antibiotic divided by the DDD (8). We observed whether antibiotics was continued or discontinued after diagnosis of CDI.
White blood cell (WBC) count, albumin and C-reactive protein (CRP) level were tested within 24 hr of enrollment to assess disease severity. Age > 60 yr, temperature > 38.3℃, albumin level < 2.5 mg/dL, or WBC count > 15,000 cells/µL got 1 point each and the pseudomembrane confirmed by endoscopy or admission in the intensive care unit got 2 points each. Sum of points was assessed as severity score of CDI and considered to have severe CDI with ≥ 2 points (9). Stool character and frequency, abdominal pain and tenderness, and laboratory findings were observed within 24 hr after inclusion.
Clinical cure was defined as resolution of diarrhea within the treatment period. Clinical failure was defined as the need for treatment change for the resolution of diarrhea. Resolution of diarrhea required conversion to two or fewer semiformed or formed stools/day (10). Recurrence was defined as growth of C. difficile with toxin genes, positive toxin assay A&B, or pseudomembrane on endoscopy with resurgence of symptoms after cessation of treatment, at least 10 days after the first episode (11). Global cure was defined as patients who were cured clinically and did not have a recurrence.
Isolates of C. difficile
Stool specimens were grown anaerobically on C. difficile Moxalactam-Norfloxacin-Taurocholate agar (CDMN-TA, Oxoid Ltd., Cambridge, UK) supplemented with 7% horse blood after alcohol shock (12). Colonies of C. difficile were identified by Rapid ID 32A (BioMerieux SA, Marcy l'Etoile, France).
Multiplex PCR for toxin gene detection
With template DNA, multiplex PCR was performed as described elsewhere with minor modification (13). Gels were run under standard condition on 1.0% agarose for 25 min and stained with ethidium bromide for visualization. The size of toxin gene tcdA, tcdB, cdtA, and cdtB was 629, 410, 221, and 262 bp, respectively.
Toxinotyping for tcdA gene
Positive results of tcdA by multiplex PCR meant intact A2 fragment of C. difficile, which did not code for production of A toxin. To confirm the production of A toxin in organism, toxinotyping for A3 PCR fragment of C. difficile was performed as described elsewhere (14). After amplication and subsequent digestion of A3 PCR product with restriction enzyme EcoR I, digests were visualized on 1.5% agarose gel. According to the type of restriction patterns, we figured out whether isolates had toxin A-producing gene or not.
Statistical methods
SPSS version 13.0 for Windows (SPSS, Chicago, IL, USA) was used for statistical analysis. Categorical variables were analyzed by Pearon's chi-square test or Fisher's exact test. Continuous variables were analyzed by independent t-test or Mann-Whitney U-test. A P value of < 0.05 by two-tailed test was considered statistically significant.
RESULTS
During the study period, 200 cases were diagnosed as CDI and 215 isolates were cultured from stool. In brief, 151 cases were CDI with isolation of toxin-producing C. difficile from stool, 49 were diagnosed by non-culture method, 18 were toxigenic carrier and 46 were non-toxigenic carrier (Table 1). For the acquisition of CDI, 11 (5.5%) were CO-CDI and 189 (94.5%) were HA-CDI.
Incidence of CDI and AAD
Incidence was reckoned from Feb 2009 to Jan 2010 because we set up the standard culture method on Jan 2009.
Total number of AAD was 769 during 1 yr. The mean number of AAD by month was 64 (range, 56-76). The mean incidence of AAD per 100,000 patient-days and 10,000 admissions by month was 313.3 and 326.6, respectively (range, 268.7-378.8 and 278.9-400). During the same period, total number of CDI was 176. The mean number of CDI by month was 15 (range, 11-24). The mean incidence of CDI per 100,000 patient-days and 10,000 admissions by month were 71.6 and 64.9, respectively (range, 52.5-114.0 and 45.0-109.6) (Fig. 1). The ratio of CDI to AAD was 0.23.
Distribution of toxigenic C. difficile isolates
The distribution of toxigenic C. difficile strain was classified by clinical diagnosis in Table 2. Among 169 toxin-producing isolates, the most common type was tcdA-positive tcdB-positive cdtA/B-negative strain (A+B+CDT-) (131/169, 77.5%). Twenty-six isolates (15.4%) were tcdA-negative tcdB-positive cdtA/B-negative strain (A-B+CDT-), and tcdA-positive tcdB-positive cdtA/B-positive strain (A+B+CDT+) comprised 7.1% (12/169). Distribution of toxigenic isolates did not show a difference among HA-CDI, CO-CDI and toxigenic carrier (P = 0.929).
Clinical characteristics
Demographic data, previous medication history, and clinical and laboratory characteristics of CDI were presented in Table 3. Medication history was obtained from 187 CDI because record of antibiotics prescription was not available in 9 CO-CDI and 4 HA-CDI cases. The most common antibiotics used previously were extended-spectrum cephalosporins (106, 56.7%), followed by respiratory fluoroquinolone (67, 35.8%) and then beta-lactam/beta-lactamase inhibitor (61, 32.6%). There was no history of antibiotic use in 2 CO-CDI and 3 HA-CDI cases.
Severity score of CDI was 1.55 ± 1.337 (mean ± S.D.), and 37.5% (75/200) was severe CDI based on severity score (score ≥ 2). Of 6 factors of severity score, age (64%) was the most common contributing factor for severe CDI.
Loose to watery character of stool was more common than mucoid stool: 155 (77.5%) vs 45 (22.5%). Number of stool passage more than 10 times per day was observed in 35 CDI (17.5%).
Clinical course and outcome of CDI
Among 200 CDI, 5 were lost before or during treatment and 6 expired due to underlying disease before treatment, therefore clinical course of 189 were observed. Diarrhea stopped without treatment in 49 cases (49/189, 25.9%). Self-remitting 49 CDI were observed through Jan 2011 at their follow-up clinic or admission and mean follow-up period were 281 days (range, 12-712). Among 49 CDI, 4 cases (8%) re-experienced diarrhea during observation period with positive toxin assay A&B, and their mean interval between diarrheal episodes were 147 days (range, 60-207). Of 140 treated for CDI, 118 (84.3%) were clinical cure, 13 (9.3%) showed clinical failure, and 9 (6.4%) expired. However, only 1 of 9 patients died because of CDI, and attributed mortality was as low as 0.7% (1/140). Thirty cases recurred after the end of treatment, and mean recurrence interval was 35 days (range, 12-90). Recurrence rate was 21.4%. Of 30 recurred cases, 25 was from clinical cure group, therefore, global cure rate was 66.4% (93/140).
According to the number of CDI episode, 118 cases (84.3%) were treated for the first episode, 17 (12.1%) for the second, 4 (2.9%) for the third, and 1 (0.7%) for the fourth. Comparing between the first treatment and retreatment groups, either clinical outcome or recurrence rate showed no significant difference (P for trend = 0.958, P = 0.256, respectively).
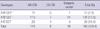
For the treatment of CDI, 123 (87.9%) were treated with metronidazole and 17 (12.1%) with vancomycin. Comparing between cases treated with each drug, there was no significant difference in clinical outcome: clinical cure, failure, mortality and attributed mortality of metronidazole and vancomycin, 83.7%, 10.6%, 5.7% and 0% vs 88.2%, 0%, 11.8% and 5.9%, respectively (P for trend = 0.912) (Table 4).
DISCUSSION
This is the first study prospectively observing the prevalence and clinical characteristics of CDI in Korea. We expect that a change of incidence or disease severity in further years could be studied based on these results, because 2 BI/NAP1/027 strains were isolated in Korea (15), and 5 more strains were discovered in this study (data not shown).
The incidence of CDI in Korea was reported variously from 8.82 to 71.71 cases per 10,000 patient admissions during the same period (3, 16). According to each study definition, 34.4% of CDI were severe cases, 47.7% of CDI patient complained of 5-7 loose stools/day, and 2.6 to 9.7% of CDI resolved diarrhea without treatment (3, 17). Relapse rate was also variable from 7% to 38.3% (17, 18). Attributable mortality was estimated 0.4%-1.3% in HA-CDI and 14.3% in severe cases (3, 19). Difference of study definition and retrospective methodology made results variable especially in incidence and relapse rate. By universal definition and prospective design of this study, these results could be compared with other countries' data and offered as baseline data.
In this study, CDI accounted for 22.8% of AAD and overall incidence of CDI was 71.6 per 100,000 patient days. The incidence of CDI in Korea (range, 52.5-114.0 cases per 100,000 patient-days) during 2009 was a little higher than that of the US (range, 3.0-7.1 cases per 10,000 patient-days) before emergence of hypervirulent strain (20). However, incidence of CDI in our hospital showed increasing tendency from November, 2009 and peaked at December, 2009 up to 2-fold higher than other months. To determine whether the incidence of CDI is increasing in our hospital, further observation is certainly necessary. Furthermore, contribution of intra-hospital spread of the organisms to the increase of CDI in non-epidemiologic setting needs to be defined in our hospital where the principle of contact precaution for CDI is not adopted.
For the acquisition of CDI, the ratio of CO-CDI to HA-CDI diagnosed during the study period was 0.06 (11/189). In Canada, the US and Europe, the ratio of CO-CDI to HA-CDI ranged from 0.23 to 0.59 (21). Although we did not actively search CO-CDI, the low proportion of CO-CDI compared with other countries suggests that there probably was few community-based outbreak or endemicity of CDI in community in Korea.
Previous studies demonstrated that approximately two-thirds of patients colonized with C. difficile become asymptomatic carrier (22), and asymptomatic carriage of C. difficile confers a low risk (approximately 1%) for subsequent CDAD, even in the presence of antibiotic therapy (23). In this study, toxigenic carrier was 10%, and 8% of them developed CDI after 60-207 days from the episode. Because stool culture was performed for the patients who have a loose stool with the use of antibiotics which did not meet the definition of diarrhea in our study, toxigenic carrier was far underestimated. For the subsequent development of CDI in toxigenic carrier, 8% is higher than expected according to the previous study (23). A recent report showed that 20% of patients with asymptomatic carriage of C. difficile developed CDI, and 60% of them were epidemic NAP1 strains (22). The authors hypothesized the reason for high incidence of CDI development in asymptomatic carriers as difference of virulence between epidemic and non-epidemic strains. We suspected that toxigenic carrier in this study might be very mild CDI patients because 25.7% of our CDI patient has a mild disease resolving spontaneously without medication.
Toxin profile of our strains was similar to the previous studies from Korea (24, 25). One study showed the increasing prevalence of A-B+CDT- strains in the early 2000s, and the percent of the strains was 39.6% in 2004. In our data, A-B+CDT- strains showed 15.4%, and those strains were identified from HA-CDI, CO-CDI and toxigenic carriers over the study period (data not shown). A-B+CDT- strains are also prevalent in Japan or China; there were 3.4%-5.6% of A+B+CDT+ strains, 12.7%-22.3% of A-B+CDT- strains, and 74.3%-81.7% of A+B+CDT- strains between 1999 and 2008 in Japan (26), and A-B+- strains comprised 33.3% in Shanghai (27). On the contrary, the prevalence of those strains in Europe, Canada or Australia was as low as 0%-6.3%, 2.4%, and 1.1%, respectively (28, 29). High prevalence of A-B+- strains in Asia is an interesting finding, which might suggest the spread of the organisms by common food transported internationally as well as heavy traffic of people among 3 countries.
Prior exposure to antibiotics varied in our study as expected. Use of clindamycin and the third generation cephalosporin was the most commonly associated with CDI (5), but exposure to antecedent fluoroquinolone has been a risk factor most prone to induce CDI recently (30). Increased fluoroquinolone usage and fluoroquinolone resistance of C. difficile strain had associated with epidemic spread of CDI caused by hypervirulent strain (1). In other study, the resistance rate to moxifloxacin of C. difficile was 42% (24). The MICs of fluoroquinolones were slightly higher for A-B+CDT- strains than A+B+CDT- strains (25). In this study, respiratory fluoroquinolone was the second most common antibiotics prescribed before CDI episode. Further observation for susceptibility of respiratory fluoroquinolone in C. difficile isolates is mandatory.
Recurrence rates after treatment with metronidazole or vancomycin are similar (1). In this study, recurrence rate of vancomycin was higher than metronidazole (41.2% vs 18.7%, P = 0.054). Our hospital strategy for treatment of CDI was that vancomycin is superior to metronidazole as the first-line agent for patients with severe CDI according to previous studies (1, 9). Severe CDIs were more included in vancomycin treated group than metronidazole treated group (52.9% vs 21.1%, P = 0.009). For the comparison of recurrence rate between treatments, multivariate analysis was done and there was no significance in statistic (OR, 2.656; 95% CI, 0.86-8.208; P = 0.09) (data not shown).
In this study, recurrence rate after vancomycin and metronidazole treatment were 41.2% and 18.7%, respectively. CDI severity score was different statistically between vancomycin treated group and metronidazole treated group (2.71 ± 1.532 vs 1.62 ± 1.277, P = 0.002). Severe CDIs were more included in vancomycin treated group than metronidazole treated group (52.9% vs 21.1%, P = 0.009). For the comparison of clinical outcome between treatments, severity score should be adjusted before analysis. Multivariate analysis was done to adjust severity score in recurrence rate according to treatment and there was no significance of treatment in statistic (OR, 2.656; 95% CI, 0.86-8.208; P = 0.09) (data not shown).
In conclusion, the incidence of CDI in Korea is 71.6 per 100,000 patient days, a little higher than other reports during the non-epidemic setting. Incidence and clinical severity as well as toxin type indicate no evidence of outbreak by hypervirulent BI/NAP1/027 strain in Korea. We expect that the change of epidemiology and clinical severity in CDI can be evaluated based on these results. Continued research into the epidemiology and disease severity is mandatory.



 XML Download
XML Download