

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
X-linked inhibitor of apoptosis protein (XIAP) is a member of the Inhibitor of Apoptosis (IAP) protein family that selectively binds and inhibits caspases-3, -7, and -9. XIAP blocks the downstream portion of the apoptosis pathway and inhibits cell death in response to multiple stimuli (1-3). All cells have a finite lifespan, and cell death occurs mainly as a result of passive necrotic processes and/or active apoptosis (programmed cell death) (4, 5). Apoptosis is the most common mechanism by which the body eliminates damaged or unnecessary cells without local inflammation from leakage of cell contents (6, 7). This process relies on a tightly balanced signaling pathway involving both pro- and anti-apoptotic proteins. Defective apoptosis represents a major causative factor in the development and progression of cancer (8). The IAP protein family plays critical roles in maintaining tight apoptogenic regularities.
XIAP expression is increased in a number of human malignancies, including colorectal, esophageal, ovarian, renal cell, hepatocellular, and prostate cancer (2). Several reports have confirmed higher XIAP expression in thyroid cancer, compared to benign thyroid disorder (9). Moreover, a recent study showed the utility of XIAP expression as a marker to predict the aggressiveness of papillary thyroid carcinoma (PTC) (10).
In the present study, we evaluated the expression patterns of XIAP in various neoplastic thyroid disorders. We additionally aimed to delineate possible associations between XIAP expression and clinicopathologic parameters in conventional PTCs, the most common type of thyroid cancer.
MATERIALS AND METHODS
Thyroid samples
We analyzed 217 formalin-fixed, paraffin-embedded thyroid tissue specimens obtained with thyroidectomy at the Asan Medical Center between 1996 and 2003. The study specimens comprised 164 conventional PTCs and 40 other malignant thyroid tumors, including 10 follicular variant PTCs, 8 follicular thyroid carcinomas (FTC), 8 medullary thyroid carcinomas, 8 poorly differentiated thyroid carcinomas and 8 anaplastic thyroid carcinomas. The remaining 13 specimens were benign thyroid tumors, including 6 nodular hyperplasia and 7 follicular thyroid adenomas.
All thyroid specimens were stained using hematoxylin and eosin, and reviewed by two pathologists. Diagnosis was confirmed according to the World Health Organization histologic classification of thyroid tumors.
Immunohistochemical analysis of XIAP
Sections of formalin-fixed, paraffin-embedded tumor tissue specimens were deparaffinized, treated with 3% hydrogen peroxide to block endogenous peroxidase activity, and microwaved in 0.01 M/L citric acid (pH 6.0) for 6 min at 100℃, followed by slow cooling for antigen retrieval. Slides were incubated for 72 hr at 4℃ with a monoclonal anti-XIAP antibody (BD Biosciences, Franklin Lakes, NJ, USA), stained using Envision-Plus reagents (DAKO, Carpinteria, CA, USA) and diaminobenzidine as chromogen, and counterstained with hematoxylin.
The extent of staining was graded semiquantitatively as follows: no foci (0), rare-few foci (1+), multiple foci (2+), and regional-diffuse staining (3+). Staining intensity was graded semiquantitatively as follows: negative (0), weak (1+), moderate (2+), and strong (3+). Specimens were classified as XIAP-positive when the sum of the extent score plus intensity score was equal to more than 4 points (Fig. 1).
Clinicopathologic features of conventional papillary thyroid carcinoma
Patients diagnosed with conventional PTC and subjected to thyroid surgery at Asan Medical Center between 1996 and 1998 were retrospectively analyzed. Demographic data, including age and gender, and pathologic data, such as tumor size, multifocality, extrathyroidal invasion and AJCC TNM 2002 staging, were reviewed.
Statistics
Categorical variables are presented as numbers and percentages, and continuous variables as means ± standard deviations or median values with a range. Comparison of clinicopathologic parameters according to positivity of XIAP expression was performed using the Student's t test for continuous data and Fisher's exact test for categorical data. All P values were two-sided. Data were considered statistically significant at P < 0.05. R version 2.11.1 and R libraries car and Cairo were used to analyze data (R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org) (11).
RESULTS
XIAP expression in malignant and benign thyroid tumors
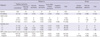
Among the 164 conventional PTC specimens, 128 (78%) stained positive for XIAP (Table 1). In terms of staining extent, 130 (82%) specimens scored 2+ or 3+. Intensity scores of 1+, 2+, and 3+ were conferred to 31 (19%), 81 (49%), and 27 (16%) specimens, respectively.
Positive XIAP staining was found in 2 (20%) of 10 follicular variant PTCs, 2 (25%) of 8 FTC, 3 (38%) of 8 medullary thyroid carcinomas, 4 (67%) of 6 poorly differentiated thyroid carcinomas, and 3 (38%) of 8 anaplastic thyroid carcinomas.
Among the benign thyroid nodule specimens, none of the 6 nodular hyperplasias and only one of 7 (14%) follicular thyroid adenomas displayed XIAP-positive staining.
Clinicopathological factors of classic PTC according to positivity for XIAP expression
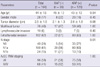
Among the 128 patients in the XIAP-positive group, 35 (27%) were in the N0 stage, 80 (63%) in the N1a stage and 11 in the N1b stage (Table 2). Among the 34 patients in the XIAP-negative group, 5 (14%) patients were in the N0 stage, 20 (56%) in the N1a stage and 11 (33%) in the N1b stage. The incidence of metastasis to lateral neck lymph node was higher in patients with negative XIAP expression than those positive for XIAP (P = 0.01).
No significant differences in age, sex, tumor diameter, multifocality, lymphovascular invasion, extrathyroidal extension, lymph node metastasis, and AJCC TNM 2002 stage were observed between the two groups.
DISCUSSION
The major histologic thyroid cancer types are composed of differentiated thyroid carcinomas, such as PTC and FTC, and undifferentiated thyroid carcinomas, such as medullary thyroid cancer or anaplastic thyroid cancer. PTC is the predominant thyroid cancer type in most parts of the world. Thyroid fine-needle aspiration cytology (FNAC) is a standard diagnostic tool for thyroid neoplasms (12). However, diagnostic challenges of inadequate specimens and indeterminate cytology categories that fail to meet the criteria for definitive diagnosis of cancer present significant obstacles to clinicians (13, 14). Data from the present study support the potential of XIAP as a molecular marker in thyroid cancer diagnosis.
More recently, molecular diagnoses, such as galectin-3, HBME-1, cytokeratin-19 or B-type raf (BRAF) gene mutations have been introduced, but their clinical value is yet to be established (15-17). Some groups have shown that immunohistochemical testing for a combination of 2 or more markers improves the accuracy of diagnosis (18-21). In our experiments, most specimens with benign pathology stained negative for XIAP. Thus, XIAP immunostaining from FNAC specimens, in combination with other potential markers, may be promising for the differential diagnosis of thyroid neoplastic disorders.
The incidence of positive XIAP expression was higher overall in thyroid cancer, particularly in cases of conventional PTC, compared with benign thyroid nodules. These findings are consistent with other studies suggesting that XIAP contributes to tumor cell survival as an apoptosis inhibitor (2). However, XIAP immunostaining is inappropriate to differentiate between other histologic types of thyroid cancer and benign nodules. In particular, FTC and follicular adenoma, which are difficult to diagnose using cytology, showed similar patterns of XIAP expression in this study. However, the number of FTC and follicular adenoma samples analyzed was limited, and thus, a follow-up study on a larger scale is needed to evaluate the diagnostic value of XIAP expression in these diseases.
Interestingly, follicular variant PTCs, such as FTC, showed a lower incidence of positive XIAP expression than conventional PTC. Although PTC as a group constitutes tumors with favorable biologic behavior that share characteristic microscopic features, increasing evidence suggests that they represent a heterogeneous group of tumors, and specific genetic alterations influence histologic variants and tumor behavior (22). Adeniran et al. (23) reported that the molecular profile of the follicular variant PTC is close to that of FTC, with high prevalence of RAS and a very low BRAF mutation rate. Riveral et al. (24) reported that the mutational patterns of encapsulated follicular variant PTC and FTC are similar. Infiltrative follicular variant PTC displays a BRAF and RAS genotype in between FTC and conventional PTC. Encapsulated follicular variant PTC has behavioral profile similar to that of FTC, while infiltrative follicular variant PTC has an invasive and behavioral profile similar to that of conventional PTC. XIAP appears to be associated with histologic variant and clinical behavior, similar to BRAF and RAS.
We further evaluated the potential association between XIAP expression and clinicopathological factors in patients with conventional PTC. XIAP expression was negatively associated with risk of lateral neck lymph node metastasis in our study. This result was inconsistent with a recent report from China (10). In the earlier study, XIAP expression was positively associated with the presence of lymph node metastasis in PTC. Several Korean groups have shown a high prevalence of the BRAF V600E mutation (around 70%-80%) in Korea (15-17), compared with other parts of the world. Additionally, Gu et al. (25) detected the BRAF V600E mutation in 34.1% of classical PTC samples. This regional difference in the prevalence of the BRAF mutation in PTC between Korea and China could explain the discrepancy regarding the association of XIAP with neck node metastasis. Further studies are required to explore the potential interactions between BRAF and XIAP.
Moreover, controversial results have been reported with regard to the association of XIAP expression with clinical outcomes in various cancer types other than thyroid cancer. A number of studies have shown that increased XIAP is correlated with decreased survival in acute myeloid leukemia, diffuse large B-cell lymphoma, and renal cell carcinoma (26). In another study, high levels of XIAP were correlated with favorable outcomes in prostate cancer and early-stage non-small cell lung cancer (27). In the current investigation, XIAP expression was negatively associated with risk of lateral neck lymph node metastasis. Lateral neck lymph node metastasis is one of the important prognostic factors for recurrence and disease-specific mortality in thyroid cancer patients (28). Eventually, XIAP expression may be used as a surrogate marker to predict prognosis in thyroid cancer.
The possible mechanisms linking XIAP expression to clinical outcomes have been explored. The anti-apoptotic activity of XIAP is regulated by Smac/DIABLO. This protein is normally localized to mitochondria and released into the cytosol during the early stages of apoptosis, where it promotes caspase activity by inhibiting XIAP. Recent studies have reported that the relative proportion of XIAP, compared with Smac/DIABLO, rather than absolute value of XIAP expression, may determine tumor cell survival (27, 29, 30). However, the present investigation focused solely on XIAP expression, and follow-up studies are required to establish the roles of XIAP and Smac/DIABLO in tumorigenesis and metastasis of thyroid cancer.
In conclusion, immunohistochemical staining for XIAP as a potential novel molecular marker may aid in differential diagnosis of thyroid cancer. Furthermore, high XIAP expression in conventional PTC is strongly associated with reduced risk of lateral neck lymph node metastasis.

 XML Download
XML Download