

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tamoxifen is a widely used selective estrogen receptor modulator (SERM) in hormone receptor positive breast cancer patients, and adjuvant tamoxifen therapy almost reduces the annual recurrence rate by half and the mortality rate by one third (1).
The biotransformation of tamoxifen is mainly mediated by cytochrome P450 (CYP) family 2, subfamily D, polypeptide 6 (CYP2D6) and CYP family 3, subfamily A, polypeptide 4/5 (CYP3A4/5) (2). Tamoxifen itself has a low affinity to estrogen receptors, but its active metabolite forms, 4-hydroxytamoxifen and 4-hydroxy-N-desmethyltamoxifen (endoxifen) mainly mediated by CYP2D6, are more potent than tamoxifen in its antiestrogenic effect (3-6). Therefore, activity of CYP2D6 is important in order to determine steady-state plasma concentrations of endoxifen and 4-hydroxytamoxifen (7). The activity of CYP2D6 varies according to the genetic polymorphisms of CYP2D6 of which allele distribution is different among ethnic groups (8). In Western countries, the CYP2D6*4 allele that may predict a lack of CYP2D6 activity exists in about 20% of Caucasians. CYP2D6*4 variants showed poorer clinical outcomes in adjuvant tamoxifen therapy than wild-type (WT) (9, 10). CYP2D6*10 variants, instead of CYP2D6*4 variants, are commonly observed in Asians (11, 12), and those genotypes have been considered a potential factor for tamoxifen resistance in Asians. A few studies are available that determine whether the genetic polymorphisms of CYP2D6 influences the outcomes of adjuvant tamoxifen therapy in Asian populations. However, those studies are limited because they only investigated CYP2D6*10 genotypes instead of sufficient identification for other CYP2D6 genotypes (7, 13, 14).
Therefore, we evaluated various genetic polymorphisms of CYP2D6 and compared the treatment outcome to the polymorphism of CYP2D6 in Korean breast cancer patients with adjuvant tamoxifen treatment.
MATERIALS AND METHODS
Participants and endpoints
The blood samples of 766 patients with breast cancer who underwent surgery at Severance Hospital, Yonsei University Health System were enrolled and evaluated for the genotyping study. Their blood samplings were obtained between 2002 and 2008.
In survival analysis, we excluded the patients with stage IV disease at diagnosis, unknown endocrine therapy, non-tamoxifen endocrine therapy, previous cancer history, unknown hormone receptor status or negative hormone receptor status, unknown metabolizers, bilateral breast cancer cases, and late sampling during the follow-up after surgery in the analysis of clinical outcomes. As such, 110 of 766 patients with hormone receptor positive primary breast cancer who underwent surgery and adjuvant tamoxifen therapy between 2002 and 2004 were enrolled for survival analysis, and all those 110 blood samples were prospectively collected at the time of definitive surgery. The dose of tamoxifen therapy was 20 mg/d, and the mean duration of tamoxifen therapy was 3.9 yr.
DNA was obtained from the blood samples using GeneAll Exgene blood SV (Geneall Biotechnology, Seoul, Korea) according to the manufacturer's protocol and stored at -80℃ in a deep freezer until the identification of the genotypes. The patients' clinicopathologic characteristics and survival data were obtained retrospectively by reviewing medical records and a regular follow-up. Adjuvant chemotherapy and radiation therapy were also given by the disease condition.
The primary endpoint was recurrence-free survival (RFS), and the secondary endpoint was overall survival (OS). RFS was defined as the time from operation to locoregional recurrence, distant metastasis, or death from any cause. The occurrence of contralateral breast cancer and primary cancer other than breast cancer were censored at the time of the occurrence. OS was defined as the time from operation to death from any cause.
Ethics statement
The institutional review board of Yonsei University Health System approved this study (4-2009-0483). Informed consents for genetic analysis in patients whose blood samples were taken before 2005 were waived by the institutional review board according to the Enforcement Decree of Bioethic and Saftey Act in Korea, and the informed consents for genetic analysis in the other patients were obtained.
Genotyping
Amplification of the CYP2D6 gene was performed using the primers 5-GTATCAGGTAGTCACAGTGGCTC-3 and 5-ACTGAGCCCTGGGAGGTAGGTA-3 with a 9700 Thermal Cycler (PE Applied Biosystems, Foster City, CA, USA), as previously described (11). Genotyping of CYP2D6 was performed by the SNaPshot method to discriminate the CYP2D6 *1, *2, *2L, *3, *4, *5, *10B (*10), *14, *18, *21, *41, *49, *52, and *60 alleles (http://www.cypalleles.ki.se/cyp2d6.htm). The details of the SNaPshot method are contained in a pending patent (PCT, KR2007/003102) (unpublished data).
To detect the deletion and duplication of the entire CYP2D6 gene, we performed two long-PCR reactions. The duplicated alleles of CYP2D6 were amplified using the primers Dup-F_2 (5'-CCT CAC CAC AGG ACT GGC CAC C-3') and Dup_R (5'-CAC GTG CAG GGC ACC TAG AT-3'). The resulting amplicon of CYP2D6 3,303 bp in length was genotyped for the presence of a duplication-specific SNP. For the entire deletion, the CYP2D6 gene was amplified using the primers CYP2D6_3 (5'-ACC TCT CTG GGC CCT CAG GGA-3') and 3'2D6*5 (5'-CAG GCA TGA GCT AAG GCA CCC AGA C-3') (15). The resulting amplicon was analyzed for the presence of CYP2D6*5-specific SNP. Both CYP2D6 duplication and deletion alleles can be discriminated by the allele-specific SNPs located within the recombinant regions. PCR was performed using a 9700 Thermal Cycler (PE Applied Biosystems) with the following conditions: initial denaturation at 94℃ for 1 min, followed by 35 cycles of 98℃ for 20 sec, 64℃ for 30 sec, 72℃ for 3 min 30 sec, and a final elongation step at 72℃ for 10 min.
Hormone receptor and HER2/neu status
Estrogen receptor (ER), progesterone receptor (PR), and HER2/neu expressions of primary breast cancer were consecutively evaluated from formalin-fixed, paraffin-embedded whole sections of surgically resected breast cancer specimens using immunohistochemistry (IHC). The cut off value for ER and PR positive was over 10% staining in IHC. An IHC score of three positive was defined as positive for HER2/neu overexpression.
Grouping of metabolizing activity and statistics
CYP2D6 predicted phenotypes were based on the genotypes by the activity score (AS) suggested by previous studies (8, 16). The cases were categorized into three groups: the extensive metabolizer (EM) group if their sum of AS was ≥ 2, the intermediate metabolizer (IM) group if their sum of AS was 1 to < 2, and the poor metabolizer (PM) group if their sum of AS was < 1, as described elsewhere (17).
One-way ANOVA was used for comparing the means of continuous variables among the EM, IM, and PM groups. A two-sided, Pearson's chi-square test or Fisher's exact test was used for analyzing of the categorical variables among the three groups. The incidence of CYP2D6 metabolizer groups in the current study was compared with that of the previous study, which was reported by Ramon y Cajal et al. (18). The statistical comparison between the two studies according to AS was performed with chi-square test using weighted cases.
The effects of CYP2D6 predicted phenotypes on RFS and OS were evaluated by the Kaplan-Meier method and log rank test. A Cox-proportional hazard model was used to determine factors associated with RFS. A P value less than 0.05 was considered as a statistically significant level. The statistical analysis was carried out using PASW statistics 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The mean age of the 766 patients at diagnosis was 47.9 yr (range, 20-86 yr). Two hundred and eighteen of the 766 patients (28.5%) were *1/*10 and it was the most common CYP2D6 genotype in the current study. This is followed by *10/*10, *1/*1, *2/*10, *1/*2, and *5/*10, showing a frequency of 143 (18.7%), 102 (13.3%), 75 (9.7%), 60 (7.8%), and 42 (5.5%), respectively. When we compared the frequency of CYP2D6 genotypes in the current study with that in healthy Korean people reported in a previous study (11), the frequency of the major genotypes between the two groups was similar (Table 1). The frequency of other genotypes in the current study is shown in Table 1. There were only two patients of the heterozygous *4 genotype in this study. The frequencies of PM, IM, and EM were 6.7%, 69.0%, and 24.3%, respectively, and the frequency of the metabolizer groups according to AS was compared with that of Western breast cancer patients (Table 2) (18). We were not able to categorize 30 patients due to their unknown CYP2D6 activity.
After the exclusion of 30 patients with unidentified metabolizers, the clinicopathologic characteristics including age, T-stage, Stage IV disease at diagnosis, histologic grade, ER, PR, and HER2 in 736 patients were not significantly different between the three groups. While 47 patients with EM genotype (26.9%) and 177 patients with IM genotype (35.9%) had shown axillary lymph node metastasis, 28 patients with PM genotype (58.3%) had axillary lymph node metastasis. The axillary lymph node metastasis was more frequently observed in the PM groups than in the IM and EM group, and the difference was statistically significant (Table 3).
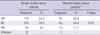
In the analysis of clinical outcomes, we evaluated 110 patients whose blood samples were collected at the time of surgery. The mean age of the 110 patients was 43.6 yr (range 26-60 yr). The clinicopathologic characteristics including age, neoadjuvant and adjuvant chemotherapy status, operation type, histologic grade, ER, PR, HER2, and status of extended or switching to AI therapy were not significantly different among the EM, IM, and PM groups, except for the T-stage and nodal metastasis. While 11 patients (42.3%) in the EM group and 23 patients (30.3%) in the IM group showed T2 cancer, six patients (75.0%) in the PM group had T2 cancer. The EM and IM groups showed 30.8% and 25.0% of axillary lymph node metastasis rates, respectively, whereas the axillary lymph node metastasis rate of the PM group was 87.5%. The difference in the T-stage and nodal status among EM, PM, and IM was statistically significant (T stage; P = 0.02, nodal status; P = 0.001). Recurrence occurred in two patients in the EM group (7.7%), six patients in the IM group (7.9%), and three patients in the PM group (37.5%), respectively. Death events were reported in two patients in the IM group (2.6%) and two patients in the PM group (25.0%), respectively. The frequency of RFS and OS events among the three groups were significantly different (RFS events; P = 0.04, OS events; P = 0.03) (Table 4).
With a median of 74 months of follow-up period (range, 4-85 months), five year RFS of the EM, IM, and PM group were 91.3%, 94.2%, and 62.5%, respectively. The Kaplan-Meier survival curves illustrated no significant difference in RFS and OS between the EM and IM groups (P = 0.96) (Fig. 1). The curves of RFS and OS of the PM group showed poorer than those of the other groups, respectively, and it was statistically significant (EM vs PM in RFS; P = 0.02, IM vs PM in RFS; P = 0.01, EM vs PM in OS; P = 0.01, IM vs PM in OS; P = 0.008) (Fig. 1).
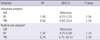
Table 5 summarized the hazard ratio (HR) and 95% confidential interval (CI) according to CYP2D6 polymorphisms. The univariate analysis using the Cox regression model showed that IM was not a risk factor for tamoxifen resistance (HR 1.06, 95% CI 0.21-5.25, P = 0.94), but PM was a high risk factor for tamoxifen resistance, and it was marginally significant (HR 5.59, 95% CI 0.93-33.5, P = 0.05). However, the multivariate analysis adjusted for metabolizer groups, age, T-stage, nodal status, adjuvant chemotherapy status, and the status of extended or switching AI therapy indicated that all metabolizer groups were not a statistically significant factor associated with RFS (IM; HR 1.32, 95% CI 0.25-6.88, P = 0.74, EM; HR 5.24, 95% CI 0.70-39.13, P = 0.10).
DISCUSSION
Some researchers investigated the association between carcinogenesis and CYP2D6 genotypes, but it is still debatable (19, 20). A previous study reported no significant association of CYP2D6*10 polymorphism with breast cancer risks in Chinese patients (12). When we compared the incidence of the major CYP2D6 variants which were frequently found in this study with the previous report of a healthy population in Korea (11), the incidence of the major CYP2D6 variants in breast cancer patients was similar with that of healthy people (Table 1). This suggested that CYP2D6 polymorphisms may be not associated with the breast cancer development.
Interestingly, the incidence of nodal metastasis seemed to be related with the CYP2D6 metabolizer grouping. We observed that the PM group showed more aggressive nodal status in the present study. The Chinese study also suggested that CYP2D6*10 is associated with nodal involvements (12). This is similar with our results. There is a possibility that the variation of the CYP2D6 genotype may be associated with nodal metastasis. To validate our results, further observational studies are needed.
Genetic polymorphisms of CYP2D6 are known to be quite different among ethnic groups. In particular, the CYP2D6*10 allele is more commonly observed in Asians, while *4 allele is more frequently observed in Caucasians (21). When we directly compared the incidence of CYP2D6 metabolizers in our study with that of the Western report using chi-square test with the weighted case, the difference was statistically significant (Table 2). Previous studies demonstrated that PM are found in about 20% among Caucasian populations, and the most common allele of PM in that population is CYP2D6*4 (22). The allelic frequency of CYP2D6*4 is 20% in Europeans, 1%-2% in East Asians, and 2%-7% in Africans (22). There were only two patients carrying the *4 allele in the present study, and it was similar with the previous Japanese study reporting a rare incidence of the *4 allele (23). IM is the most common metabolizer in this study, which was mainly contributed by the *10 allele. This relatively high proportion of IM genotypes compared with European populations was similar with other reports (14, 22). Because of this ethnic difference in CYP2D6 polymorphisms and metabolic activity, the association of clinical outcomes with tamoxifen therapy could be different among ethnic groups.
Since the previous report suggested that *4/*4 genotypes tend to have a higher risk of disease recurrence (9), a few studies have been reported in which patients carrying homogenous *10 alleles in Asians are associated with a higher hazard ratio or poorer survival outcomes (7, 13, 23). In the current study, we found that IM genotypes were not related with poorer RFS compared with the EM genotypes. However, RFS of the PM group was significantly worse than that of the EM or IM group. It may be due to the fact that the PM group has more patients with a larger tumor size and more lymph node metastasis than the others, which may strongly influence the difference in RFS and OS between the PM and the EM/IM. With the multivariate analysis, no association was found between the clinical outcome and CYP2D6 metabolizers grouping, and it might suggest that CYP2D6 metabolizer activity may not be a risk factor of tamoxifen resistance. In addition, the distinct feature of CYP2D6 polymorphisms among ethnicities, the rare incidence of PM in Korean, might be a crucial factor to evaluate the effect of CYP2D6 polymorphisms. Thus, further study including a larger population that can obtain sufficient statistical power to discover the implication of the rare PM genotypes on tamoxifen resistance in Asians is necessary.
Taken together, these results are not enough to support the previous reports that suggest a positive correlation between CYP2D6 polymorphisms and treatment outcomes in patients treated with tamoxifen. Okishiro et al. (14) suggested that the CYP2D6*10/*10 genotype, that was mainly related with the IM groups in this study, was not associated with the prognosis in patients treated with tamoxifen. This supports our results. Therefore, in contrast to the effect of poor metabolizers such as the *4 allele, such a reduced level of the active metabolites caused by the metabolic activity of the IM including the *10 allele can still be effective and sufficient to suppress in vivo tumor recurrence. In addition, it is also possible that the use of chemotherapy or extended or switched AI may wash out the effect of reduced CYP2D6 activity on the prognosis. This possibility is supported by the findings that previous studies evaluating the patients with tamoxifen monotherapy showed a relatively positive finding between the CYP2D6 genotype and clinical outcome (9, 10, 23), whereas previous studies including the patients receiving combined adjuvant therapy such as chemotherapy or ovarian suppression therapy did not demonstrate an association between the CYP2D6 genotype and clinical outcomes (14, 24, 25). Furthermore, the results from ATAC and BIG-1-98 trials presented no relationship between CYP2D6 genotypes and clinical outcomes in postmenopausal women with hormone receptor positive breast cancer at the 33rd San Antonio Breast Cancer Symposium (26, 27), and the recent meta-analysis results could not demonstrate statistically significant differences according to CYP2D6 genotyping in terms of disease-free survival and OS (28). Those results correspond with our results.
This study has several limitations. First, there has been reported that the distributions of enzyme activity-genotype were different between races; for example, the CYP2D6 *1/*1 genotype is usually identified as the reference group but the mean metabolic ratio (MR) of *1/*1 for Korean was significantly lower than the MR for Caucasian (29). Thus, there may be a misclassification of predicted phenotypes of CYP2D6 based on the activity score of genotypes among Caucasian. Further study is needed to associate the enzyme activity with known genotypes for each ethnic population. Second, the effect of concomitant use of CYP2D6 inhibitors and the compliance of the use of tamoxifen seems to be a crucial factor on the clinical outcomes, and those were validated by a previous study (30). We did not identify cases with CYP2D6 inhibitors that may alter the activity of CYP2D6 and the patients' compliance regarding tamoxifen ingestion. Nevertheless, to our knowledge, this study identified various genetic polymorphisms of CYP2D6, and is one of the largest cohort studies of CYP2D6 polymorphisms in Asian breast cancer patients with adjuvant endocrine therapy to date. Furthermore, the Food and Drug Administration of the United States (FDA) has yet to reach a consensus in recommending the testing of CYP2D6 for tamoxifen treatment, even though the Roche AmpliChip CYP450® test is easily used for the determination of CYP2D6 genotypes and was approved by FDA (18).
In conclusion, it is too early to confirm that the polymorphism of CYP2D6 is associated with tamoxifen resistance in Korean or Asian populations.




 XML Download
XML Download