

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
HER-2 is an oncogene that is overexpressed and/or amplified in about one-third of breast cancer cases (1, 2). It is associated with tumor aggressiveness such as high tumor grade, lymph node metastasis, and brain metastasis (3-7). More importantly, HER-2 is a biomarker for targeted immunotherapy such as with trastuzumab (8-10). Therefore, the proper evaluation of HER-2 gene status is important for breast cancer therapy. In clinical practice, the standard method to examine HER-2 gene status is immunohistochemistry (IHC) or fluorescence in situ hybridization (FISH) (11-13). However, breast cancer is typically a heterogeneous tumor with intratumoral heterogeneity in not only histologic features, but also genetic features (14, 15). The incidence of HER-2 gene heterogeneity in invasive breast cancer is 1.3%-54% (16-21). However, the incidence of HER-2 gene heterogeneity in invasive breast cancer in Korea has not been studied. The purpose of this study was to investigate the incidence and characteristics of HER-2 gene heterogeneity in invasive breast cancer in routine FISH examination.
MATERIALS AND METHODS
Patients
This study included 972 cases of primary invasive breast cancer diagnosed between January 2008 and December 2010. We retrospectively reviewed image files from FISH studies for the HER-2 gene that had at least three images (range 3-10) per case. Clinicopathologic parameters such as age at initial diagnosis, histologic type, histologic grade, estrogen receptor status, progesterone receptor status, and HER-2 IHC results were obtained from pathology reports. The histological grade was assessed using the Nottingham grading system (22). HER-2 staining was analyzed according to the American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) guidelines using the following categories: 0 = no immunostaining; 1+ = weak incomplete membranous staining, less than 10% of tumor cells; 2+ = complete membranous staining, either uniform or weak in at least 10% of tumor cells; and 3+ = uniform intense membranous staining in at least 30% of tumor cells (23).
FISH analysis
Before FISH analysis, invasive tumors were examined on hematoxylin-eosin stained slides. FISH was subsequently performed on the tested tumor. FISH was performed using a PathVysion HER-2 DNA Probe Kit (Vysis, Downers Grove, IL, USA) according to the manufacturer's instructions. HER-2 gene copy number on the slides was evaluated using an epifluorescence microscope (Olympus, Tokyo, Japan). At least 60 tumor cell nuclei in three separate regions were investigated for HER-2 and chromosome 17 signals. HER-2 gene amplification was determined according to the ASCO/CAP guidelines. An absolute HER-2 gene copy number lower than 4 or a HER-2 gene/chromosome 17 copy number ratio (HER-2/Chr17 ratio, or amplification index [AI]) less than 1.8 was considered HER-2 negative. An absolute HER-2 copy number between 4 and 6 or a HER-2/Chr17 ratio between 1.8 and 2.2 was considered HER-2 equivocal. An absolute HER-2 copy number greater than 6 or a HER-2/Chr17 ratio higher than 2.2 was considered HER-2 positive (23). Chromosome 17 polysomy was defined as a centromeric chromosome 17 spot count of 3.0 or more in at least 80% of tumor cells (24). High-grade amplification was defined as a HER-2/Chr17 ratio higher than 5.0, and low-grade amplification was defined as a HER-2/Chr17 ratio greater than 2.2 but less than 5.0 (25, 26). HER-2 gene heterogeneity (GH) was defined as more than 5% but less than 50% of the analyzed invasive tumor cells having a HER-2/Chr17 ratio higher than 2.2, according to CAP guidelines (27).
Statistical analysis
Data were processed using SPSS for Windows, version 12.0 (SPSS Inc., Chicago, IL, USA). Student's unpaired t-test and Fisher's exact test were used to examine differences in continuous and categorical variables, respectively. Correlation analysis was performed by Pearson's method. Significance was assumed when P < 0.05.
RESULTS
Patient characteristics
Table 1 shows the clinicopathologic characteristics of the patients. Of 971 cases, HER-2 GH was observed in 24 (2.5%) cases, all of which were invasive ductal carcinoma (IDC) and showed a higher proportion of borderline or amplified HER-2 gene status than breast cancer without HER-2 GH (P < 0.001). Of 24 cases with HER-2 GH, all 14 cases with HER-2 amplification showed low-grade amplification (P < 0.001). The incidence of chromosome 17 polysomy was higher in cases with HER-2 GH than cases without (P = 0.001).
Clinicopathologic features of HER-2 genetic heterogeneity
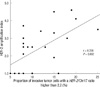
Fig. 1 shows histology, IHC, and FISH results for breast cancer with HER-2 GH. Histology was IDC, not otherwise specified (NOS) (Fig. 1A-C). Only some invasive tumor cells (arrow) showed 3+ overexpression of HER-2 (Fig. 1D-F), which was compatible with the FISH results that showed only a proportion of invasive tumor cells with a HER-2/Chr17 ratio higher than 2.2 (Fig. 1G-I). Detailed characteristics of the 24 cases with HER-2 GH are in Table 2. HER-2 gene AI rang-ed from 1.0 to 4.6, and the HER-2 GH pattern was single cell in 22 cases and cluster pattern in 2 cases. The mean proportion of invasive tumor cells with a HER-2/Chr17 ratio higher than 2.2 was 11.6% (range: 5%-25%), with significant correlation between the proportion of invasive tumor cells with a HER-2/Chr17 ratio higher than 2.2 and HER-2 AI (Fig. 2; r = 0.358 and P = 0.002). The proportion of invasive tumor cells with a HER-2/Chr17 ratio higher than 2.2 increased from the no-amplification group to the borderline group to the amplification group, but the difference was not significant (Fig. 3, P = 0.085).
DISCUSSION
This study evaluated the intratumoral heterogeneity for HER-2 in invasive breast cancer using FISH. The incidence of HER-2 GH was 2.4%, similar to the incidence of 1.3%-54% seen in previous studies (16-21). However, a simple comparison is not reasonable because study group characteristics, the number of study groups, the area evaluated by FISH, and the method of counting HER-2 signals is likely to differ among studies.
HER-2 GH can be classified into geographic heterogeneity and intercellular heterogeneity according to the method used to determine the tumor area evaluated by FISH. Geographic heterogeneity is defined as one core showing HER-2 amplification, while another shows no HER-2 amplification, when multiple tumor areas are sampled by tissue core using tissue microarray. Previous studies using this tissue microarray method showed a HER-2 GH incidences of 13%-16% (19, 21). Intercellular heterogeneity is indicated when a different HER-2 gene status is noted among invasive tumor cells evaluated in one field or focus, specifically when one microscopic field has both tumor cells with a HER-2/Chr17 ratio that is higher than 2.2 and tumor cells have a lower ratio.
In this study, image files obtained from FISH study were retrospectively reviewed, and intercellular heterogeneity rather than geographic heterogeneity was identified. A possible explanation for the lower incidence of HER-2 GH in this study could be the study method. However, we did identify HER-2 GH, even though a retrospective study design was used to examine image data from daily clinical practice. In general, breast cancer GH results from clonal diversification and differences in genetic composition from growing genetic instability in some part of the tumor (14, 28, 29). Genetic differences in a single tumor were shown by laser microdissection and a comparative genomic hybridization study, and these differences were confirmed by FISH and microsatellite instability analysis (15). Szollosi et al. (30) reported the cell-to-cell heterogeneity of HER-2 gene amplification in a FISH study of breast cancer, showing prominent heterogeneity in both the copy number of HER-2/cell and the p185HER-2 protein level, consistent with results of this study. HER-2 GH could be explained by acquisition or loss of the HER-2 gene, but HER-2 gene amplification is more plausible, considering that HER-2 is associated with tumor aggressiveness (20).
Clinically, HER-2 GH is important in the interpretation of HER-2 gene status according to FISH results and in the selection of patients for trastuzumab treatment. In this study, when HER-2 gene status was interpreted by ASCO/CAP guidelines, HER-2 GH was noted in all groups: no amplification, borderline amplification, and amplification. In addition, all cases with both HER-2 GH and HER-2 amplification showed low-grade amplification. Therefore, HER-2 GH may affect the interpretation of HER-2 amplification status results by FISH. To prevent this bias, ASCO/CAP guidelines suggest investigating at least two (and up to four) representative fields, which should be determined by scanning the entire slide (23). However, differences in the area evaluated by FISH and HER-2 signal counting method could give rise to inconsistencies in interpreting HER-2 gene status results. A previous study reported that the results of routine assessment of the HER-2 gene might be affected by breast cancer GH with low-grade amplification due to subclones of tumor cells with chromosome 17 polysomy without gene amplification (21). Another important issue in HER-2 GH is trastuzumab treatment, but whether trastuzumab treatment is potentially beneficial to patients with HER-2 GH is not known, so clinical studies are necessary. Although the clinical implications of HER-2 GH for trastuzumab treatment are uncertain, when HER-2 GH is identified, the phrase "HER-2 genetic heterogeneity is present" should be inserted in the pathology report with: 1) percentage of invasive tumor cells with HER-2 amplification; 2) pattern of amplified cells, for example scattered cells or specific clusters; and 3) pattern of specific clusters, ratio and number of chromosome enumeration probe 17 signals/cell or area and HER-2 signals/cell or area (27). In conclusion, the phenomenon of HER-2 GH in invasive breast cancer is identified in routine FISH examination, and HER-2 GH may affect the interpretation of HER-2 gene status by FISH.




 XML Download
XML Download