

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ionizing radiation (radiation) is defined as the energy required to remove electrons from a molecule (1) and a radiation worker is defined as one who is exposed or possibly exposed to radiation due to work-related activities. As in most countries, radiation is a unique toxic agent controlled by the Atomic Energy Act (Atomic Act) and Medical Service Act (Medical Act), and managed by the Occupational Safety and Health Act (OSH Act). Radiation-induced disease can be divided into radiation injury and cancer. The main cause of radiation injury is accidental overexposure that is usually reported as a skin burn.
In the latter part of the 1990s, claims for compensation of radiation-related cancer have increased. In 2000, acute myelocytic leukemia from radiation exposure was formally approved as an occupational disease (2) by the administrative courts. After the radiation-related industry was established in Korea, the first formal case of a radiation accident occurred at the Atomic Energy Research Institute in 1961 (3). From 1961 to 1969, 32 accidents were reported. Among them was a case of over-exposure up to 1.3 Sv to the entire body due to mismanipulation at a Cobalt-60 gamma irradiation facility.
According to the Korea Institute of Nuclear Safety (KINS), 27 cases of occupational radiation exposure accidents were reported from 1984 to 2005 (4), with additional radiation injury reports coming from related academic societies. Anxiety related to radiation exposure have caused many controversies for related industrial nuclear development and are a result of high profile accidents, such as the 1986 Chernobyl accident in the Ukraine and the anencephaly case of an inhabitant in Korea near the Yonggwang Nuclear Power Plant (NPP) in 1989. An epidemiological study on the NPP and nearby residents was commenced because of the anencephaly case; in addition, a follow-up study on cancer incidence and mortality is ongoing in the area. Recently, a lawsuit regarding occupation-related syndactyly was decided, with the court ruling there was no causal relationship (2008gahap6865); however, this illustrates that radiation anxiety is still a current social issue.
To investigate radiation-induced disease in Korea, we first analyzed the level of occupational radiation exposure, searched for various kinds of cases for related accidents and occupational diseases, and then estimated related and future research. It should be noted that the Ministry of Education Science and Technology (MEST), Korea Food and Drug Administration (KFDA), and the Ministry of Employment and Labor (MOEL) manage Korean radiation workers separately; therefore, it is necessary to understand the current system and recommend future changes.
MATERIALS AND METHODS
The search for articles related to Korea were restricted to English-language publications published by December 31, 2009, and was carried out using Medical Subject Heading search terms (Key words: radiation, protection, occupational exposure, nuclear power plant, Korea, Korean) of MEDLINE, a search engine of the National Library of Medicine.
In Korea, searches were conducted using the Research Information Service System, National Digital Science Links (Key words: radiation, accident, disease). Other sources for publications included individual journals such as the Journal of Korean Nuclear Society, Journal of Korean Association of Radiation Protection, Korean Journal of Dermatology, Korean Journal of Occupational and Environmental Medicine, and Journal of Preventive Medicine and Public Health; the references cited in the text of selected papers were also searched. In addition, to investigate the level of exposure and health management, research materials from KINS, MOEL, and the Occupational Safety and Health Research Institute (OSHRI) were analyzed. The workers' number of compensation claims on occupational disease predicted using the method of Jeong et al. (5).
RESULTS
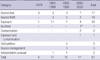
There were 62,554 occupational radiation workers in nuclear power plants, medical fields, industry, and miscellaneous positions as of 2006. The occupational categories of these workers were medical 53%, nuclear power plants 21.3%, and industry 17.5% (Table 1).
There were 8 reported cases of health disorders due to radiation accidents (except for medical fields) in Korea. The total subjects to exposure were 15 males that had radiation burns that occurred during non-destructive testing (Table 2).
Table 3 shows the distribution of major radiation accidents in Korea. The highest were the 61 radiation accidents that occurred as of 2009 that include radiation exposure and source loss cases.
Table 4 shows results of workers' compensation claims on occupational diseases. The first claim for occupational disease of a nuclear power plant worker was acute myelocytic leukemia in 1988; however, it was dismissed. In 2000, acute myelocytic leukemia of a nuclear power plant worker who had performed welding operations at the nuclear power plant was the first approved case.
Of the predicted number of compensations for occupational diseases in 2015, the approval possibility for leukemia (except chronic lymphocytic leukemia) was the highest. The numbers of approval possibility for leukemia were predicted to be 0.406, 0.472, and 0.622 at significance levels of 90%, 95%, and 99%, respectively. The significance levels for colon cancer were 0.008, 0.025, 0.115, and the respective numbers of 0.04, 0.058, and 0.622 in non-melanoma skin cancer (non-basal cell carcinoma) were predicted to receive approval as occupational diseases. The numbers of approval possibility for occupational disease in total cancers except duplicated cancers were 0.473, 0.586, and 1.003 at significance levels of 90%, 95%, and 99%, respectively. The numbers of compensation cases by 2015 also were predicted to be 3-5, 4-6, and 6-10 at the significance levels of 90%, 95%, and 99%, respectively (Table 5).
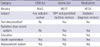
The radiation management systems are shown in Table 6. Radiation-related acts consist of the OSH Act, Atomic Act, and Medical Act. Each Act targets different subjects. The Medical Act covers health care workers exposed to radiation. The Atomic Act is applied to all workers in atomic power plants and in non-destructive testing industry. The OSH Act covers all workers exposed to radiation, but does not require to keep the record of exposure dose while the Atomic and Medical Acts do.
DISCUSSION
MEST and KFDA established databases on present occupational exposure status. Lee (6) reported on established occupational exposure levels and the unmanaged data of air-crews, as they were not yet classified as radiation workers in Korea. Upon this, KINS published a report on the radiation exposure level for the Korean population (7). As nuclear and medical radiation workers were legally required to wear a dosimeter and a dosimetry record system was legally enacted, it was possible to acquire dose information. For aircrews, even though exposure management has not been undertaken, it was possible to use a cumulative calculation program to analyze cosmic rays on some flight routes. In this study, coal miners exposed to radon and diagnostic radiography technicians at animal hospitals were excluded (7).
In 2006, there were 62,554 radiation workers, and 67% of these people were shown to have no exposure or less than 1.2 mSv per year, which was consistent with the general distribution of radiation workers (8). The exposure limit in Korea must not currently exceed 100 mSv per 5 yr and 50 mSv per 1 yr. Workers receiving a dose of more than 20 mSv totaled approximately 0.3% and showed that the exposure dose has been managed well (7). However, according to Lee et al. (9) who compiled exposure records of KFDA from 1996 to 2006, the highest exposures (classified by occupation) were for radiation technologists with an average annual effective dose of 1.83 mSv; the average of all occupational workers was 0.94 mSv. The level of radiation exposure has decreased every year and suggests that exposure management has improved.
In 1976, the only reported death by radiation exposure was caused by a safety failure at the irradiation room of the Korea Atomic Energy Research Institute (10). However, the most common injured parts of the body in radiation accidents were the hands, often due to unrecognized radiation exposure in the non-destructive testing industry (4).
There were 5 reported cases of radiation exposure in Korea that occurred during non-destructive testing, with 12 males experiencing radiation burns (Table 2). The current status of primary radiation accident in Korea has been posted on the related homepage of the KINS (rasis.kins.re.kr/) (Table 3).
Radiation is classified as a confirmed carcinogen by the International Agency for Research on Cancer (IARC). It is known that (except for mesothelioma and chronic lymphocytic leukemia), radiation causes almost all kinds of cancers (1). Due to the increase in number of radiation-related workers and the higher social recognition of occupational disease (particularly cancer), the claim for occupational disease compensation related to radiation exposure has been increasing. In 1998, a male NPP worker made a claim for compensation due to occupation-related radiation exposure causing cancer. However, this case was dismissed because there was no documented radiation exposure information according to a dose record system available. After that, an NPP welder with acute myelocytic leukemia became the first approved case, and it provided an opportunity to study the availability of probability of causation (PoC) for a scientific approach to occupational diseases (11). After the adoption of a PoC assessment for occupational diseases, the occupational disease review committee of the OHSRI has used it to discuss the causal relationship between radiation exposure and diseases. However, some unfavorable cases were later approved by the administrative courts (4).
Decision-making has become more important and the number of radiation workers and the necessity for radiation-induced occupational disease compensation has increased. Though cancer does not exhibit any special aspects related to radiation, an objective statistical measurement, the PoC, has been defined below to assess the contribution of radiation exposure to the development of cancer in a radiation worker (12).

BaseRisk refers to the baseline cancer risk of the general population, while RadRisk is the excess cancer risk due to radiation exposure. Therefore, PoC measures the rate of the cancer risk increased by radiation exposure to the total cancer risk of the population exposed to radiation; when that value exceeds 50% it was considered that the cancer was due to radiation exposure.
In 1985 (13), the National Institute of Health used PoC to assess the radiation causality of cancer in radiation workers, and the National Institute for Occupational Safety and Health (NIOSH) developed the NIOSH-Interactive RadioEpidemiological Program (www.niosh-irep.com/irep_niosh) as a PoC calculation program based on the National Cancer Institute-Centers for Disease Control model and has operated it until now (14), the US Department of Energy (DOE) is currently judging a request for radiation-induced occupational disease compensation raised by the US DOE or nuclear weapons-related workers on the basis of the 99% upper confidence limit of PoC.
In 1999, the Korea Radiation Risk and Assigned Share (KORRAS) first developed a PoC calculation program for radiation workers in Korea (15). KORRAS provided various modes of PoC point estimates, and it was suggested to use the largest estimate of PoC for a person who developed cancer. However, various uncertainties existed in the PoC calculation. Therefore, the PoC should be presented as a distribution or confidence interval that better reflects these uncertainties, rather than a single point estimate. Currently, the Radiation Health Research Institute-Program for Estimating the Probability of Causation (RHRI-PEPC) is evaluating the radiation causality of cancer in Korean radiation workers (11) that reflects background mortality, incidence, and the smoking rate in Korea; in addition, the study is based on the most recent NCI-CDC mode. RHRI-PEPC is also using a computer program developed to calculate the distribution of PoC.
It is expected that the number of radiation workers will increase continuously, leading to increased cancer incidence and mortality; as a result there is a possibility that claims for occupational disease compensation will also increase. Therefore, the social costs of occupational disease will need to be evaluated. To solve this problem, it is necessary to introduce a screening dose. The US Department of Veterans Affairs used a screening dose that considered the uncertainty of PoC on the basis of a calculation model that judged requests for radiation-induced occupational disease compensation by veterans (16). This screening dose can also be used to estimate the number of persons who may possibly be approved for future occupational disease compensation. Jeong et al. (5) proposed a screening dose through the use of exposure data of MEST and estimating the numbers of compensation cases for occupational disease. The numbers of compensation cases that would be approved as occupational disease for the next decade were predicted to be 3-5 workers, 4-6 workers, and 6-10 workers at the significance levels of 90%, 95%, 99%, respectively.
A cohort study of NPP workers and nearby residents was started in 1992 to comprehensively verify the hypothesis of the study: 'Can the operation of NPP casually increase the incidence risk in nearby residents and workers?' (17). This study was conducted by Seoul National University and supported by MEST. The cohort was included in the international collaborative study of cancer risks among workers in the nuclear industry (8). The follow-up on cancer incidence and mortality for NPP nearby residents (n=10,548) and the control group (n=23,041), and NPP workers (n=8,552), and the control group (n=9,096) will be finished in 2011 (17). In contrast, the epidemiological study for all Korea NPP workers was finished by the Radiation Health Research Institute; the results did not show an increase in cancer incidence or mortality according to radiation exposure dose until now (2, 18, 19).
The increase in requests for radiation-induced cancer compensation led to a recent health status survey for radiation workers conducted by the OHSRI in Korea (4). The study showed that the incidence of thyroid cancer in radiation workers may be higher than other occupations through the use of MEST radiation worker exposure data and National Health Insurance Corporation admission data (20). However, it cannot exclude the mass screening effects and further study will be needed.
The KFDA manages medical radiation workers and established a cohort study using exposure records (21). Lee et al. (9) arranged exposure records by using the KFDA database from 1996 to 2006. Radiation technologists were exposed to a relatively high radiation dose and the average annual effective dose was 1.83 mSv; the average of whole subjects were 0.94 mSv.
Korean radiation workers are regulated by three acts, the Atomic Act, the Medical Act, and the OSH Act. However, there were some mismatches or non-organized points for the exposure measurement and health management. Recently, Kim (22) made some suggestions following a health management survey of radiation workers: 1) Radiation measurement is regulated by the Atomic Act and Medical Act, so the OSH Act can follow these acts and 2) Health management of radiation workers, that includes health examinations and education, should be organized by the Medical Act.
The OSH Act needs to reestablish health management to the notified user. At present, the OSH Act designates general management, including health education and a special health examination to the notified user. However, the Atomic Act has no special regulation because the exposure level was very low (22). Therefore, Kim (22) suggested that the Atomic Act would be more applicable. There are currently no regulations for air-crews and veterinary hospital radiation workers and the above criteria should be applied to them. The occurrence of radiation and accidents will most likely decrease if a consistency can be maintained.
Radiation-induced disease can be divided into radiation injury and radiation-induced cancers; it is expected that these injuries will be reduced in the future. However, the cancer mortality for 65 yr-old Korean men was 27.7% in 2008 (23) and is expected to remain the same in the future (24). This situation will lead to a drastic increase in claims for occupational disease compensation. Therefore, establishing a scientific and objective judging system using PoC and screening dose would save social costs and better judge the work related occupational disease. In addition, the radiation-related acts that have not been consistently managed need to be rearranged and reestablished, with a reorganization of the exposure assessment, record system, and health surveillance system for all radiation workers.




 XML Download
XML Download