

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bloodstream infection (BSI) is potentially life-threatening condition with a case fatality rate of 30-40% (1). If BSI is clinically suspected, clinicians should choose antibiotics based on the type of infection, underlying disease, patient age, infecting pathogen, and site of acquisition of infection (2).
BSI can be classified as community-acquired (CA), hospitalacquired (HA), or healthcare-associated (HCA) depending on the site of acquiring infection and risk factors. Of 3 epidemiologic categories, HCA-BSI is a recently developed category that is traditionally classified as CA-BSI (3-5).
Clinically, the characteristics of HA-BSI can be separated from those of CA-BSI in many factors such as pathogen distribution, type of infection and their susceptibility patterns. Staphlylococcus and catheter-related infection were predominant in HA-BSI, while Escherichia coli and urinary tract infection were generally predominant in CA-BSI (6-8). With regard to HCA-BSI, previous studies showed that the clinical characteristics were not similar to those of CA-BSI (3, 5, 9). And the susceptibility patterns of HCA-BSI were similar to those of HA-BSI (5, 9). Generally, the concept of HCA-BSI has been accepted to be an independent epidemiologic category of BSI. However, so far the detailed data of clinical characteristics of HCA-BSI were not sufficient. Also, the independent risk factors for mortality of each BSI have not been compared yet.
In this study, we compared clinical characteristics of 3 BSI groups including HCA-BSI, instead of investigating one pathogen or one source. And we performed additional analysis to evaluate risk factors for mortality according to the epidemiologic type of infection.
MATERIALS AND METHODS
Study design and data collection
This study was a prospective nationwide surveillance of BSI in 9 university hospitals in various regions of Korea from October 2006 to September 2007. The participating institutions included Kyunghee East-West Neo Medical Center (800-bed, Seoul), Samsung Medical Center (1,270-bed, Seoul), Kangbuk Samung Hospital (620-bed, Seoul), Konkuk University Hospital (820-bed, Seoul), Kyungpook National University Hospital (850-bed, Daegu), Keimyung University Dongsan Medical Center (910-bed, Daegu), Chungnam National University Hospital (980-bed, Daejeon), Chonnam National University Hospital (850-bed, Gwangju), and Jeju National University Hospital (300-bed, Jeju). The following data were collected from all cases of BSI; demographic information, underlying disease, comorbid conditions, microbiological data, sources of infection, and other important clinical parameters at the time of infection. The main clinical outcome was measured by the 30-day mortality rate.
Study population
All blood isolates during the study period from the participating hospitals were reviewed for clinical significance. Cases that showed clinical features of Systemic Inflammatory Response Syndrome (SIRS) were included in this study. SIRS was defined by the presence of at least two of the following signs and symptoms: tachycardia (pulse rate >90 beats/min); tachypnea (respiratory rate >20/min); fever (body temperature >38℃) or hypothermia (body temperature <36℃); leukocytosis (white blood cell count >12,000 cells/µL) or leukopenia (white blood cell count <4,000 cells/µL) (10). The site of infection causing BSI was estimated by infectious disease specialist at participating institutions. All underlying diseases and comorbid conditions for each patient were included in the analysis. And only the first bacteremic episode for each patient was included.
Definitions
BSI cases were classified as CA, HA, or HCA depending on the site of acquiring infection and risk factors. HA-BSI was defined if blood culture was positive >48 hr from admission or who had been discharged from an acute care hospital within the past 10 days. HCA-BSI was defined if patients had a history of hospitalization for 2 or more days in the previous 90 days; receipt of intravenous (IV) medication or home wound care in the previous 30 days; receipt of hemodialysis; or residence in a nursing home or long-term care facility (3, 5, 9). CA-BSI was defined if patients had the first positive blood culture <48 hr after admission and who did not have any risk factors for HCA-BSI. Neutropenia was defined as an absolute neutrophil count below 500/µL. Corticosteroid use was noted only if the patient had recently received the equivalent of 30 mg of prednisone daily for at least seven days, or 20 mg each day for 14 days. Receipt of immunosuppressant was defined as use of any immunosuppressive drug (e.g., cyclosporine, antineoplastic chemotherapy) in the previous 30 days. Prior antibiotic use was defined as use of antimicrobial agent for >3 days in the previous 30 days. High alcohol uptake was noted if the patient had ingested >100 g of alcohol every day. Severe sepsis was defined as sepsis associated with the presence of at least one or more following signs of organ dysfunction; metabolic acidosis, acute alteration in mental status, oliguria, and/or adult respiratory distress syndrome (11). The Pitt score was calculated within 2 days prior to or on the day of first positive blood culture on the basis of 5 parameters (fever, hypotension, mechanical ventilation, cardiac arrest, and mental status) (12). The initial empirical antibiotic therapy was considered 'appropriate' if the initial antibiotics, which were administered within 24 hr after acquisition of blood culture samples, included at least one antibiotic that was active in vitro and when the dosage and route of administration confirmed with current medical standards. Otherwise, initial antibiotic therapy was considered 'inappropriate' (13). The 'improvement' of treatment outcome was defined as partial resolution of presenting signs and test results (e.g., fever, elevated leukocyte) of the infection (14).
Microbiological tests
All isolates identified from each hospital were transported to the central laboratory of the Asian-Pacific Research Foundation for Infectious Diseases (ARFID), Seoul, Republic of Korea. Antibiotic susceptibility testing was performed in this laboratory using the modified broth microdilution method. Minimum inhibitory concentration (MIC) breakpoints and quality control protocols were used according to the standards established by the Clinical and Laboratory Standards Institute (CLSI) (15).
Statistical analysis
Student's t-test was used to compare continuous variables (age and PITT score), and chi-square or Fisher's exact test was used to compare categorical variables (underlying diseases, comorbid conditions, microorganism distributions, sources of infection, and treatment outcome). For pairwise comparisons, 3×2 table (3 epidemiologic type of BSI) was broken down into three 2×2 tables (CA vs. HCA, HA vs. HCA, CA vs. HA). To determine the independent risk factors for mortality, a multiple logistic regression analysis was used. P values <0.05 were considered statistically significant. The SPSS for Windows software package (version 11.5) was used for this analysis.
RESULTS
Patient characteristics
A total of 1,605 blood isolates were obtained from 9 hospitals between October 2006 and September 2007. Of these 1,605 isolates, 461 isolates (28.7%) were not considered true pathogens because there were no compatible clinical features of SIRS. Among 1,144 isolates included in the study, HA-BSI accounted for 48.8% (558/1,144), CA-BSI for 33.2% (380/1,144), and HCA-BSI for 18.0% (206/1,144).
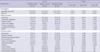
The mean age was the highest in patients with CA-BSI (57.0±20.7), followed by HCA-BSI (53.7±20.7), and HA-BSI (47.3±23.7) (Table 1). With regard to underlying diseases, solid tumor and hematologic malignancy was the most common disease in HCA-BSI group (54.9%) and HA-BSI group (24.6%), respectively. Compared with other groups, patients with CA-BSI were significantly less likely to have solid tumor (24.2%, 32.4%, 54.9% in CA-BSI, HA-BSA, and HCA-BSI, P<0.005, respectively) and hematologic malignancy (3.4%, 24.6%, 16.0% in CA-BSI, HA-BSA, and HCA-BSI, P<0.005, respectively).
Patients with HA-BSI or HCA-BSI were more likely to have severe comorbidities (neutropenia, receipt of steroids, receipt of immunosuppressant, or prior antibiotic use) compared with CA-BSI group (for neutropenia, 8.9%, 28.3%, 25.2% in CA-BSI, HA-BSI, and HCA-BSI, P<0.005; for receipt of steroid, 4.7%, 28.1%, 24.3%, P<0.005; for receipt of immunosuppressant, 9.2%, 33.2%, 31.6%, P<0.005; for prior antibiotic use, 7.1%, 54.7%, 14.6%, respectively, P<0.005).
Pathogen distribution
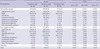
Of all BSI isolates, 59.2% were Gram-negative aerobes, and 38.9% were Gram-positive aerobes. As a total, E. coli (27.8%) was the most common isolate followed by Klebsiella pneumoniae (13.6%), S. aureus (12.4%), coagulase-negative Staphylococcus (9%), Enterococcus species (7.1%) (Table 2). The prevalence of E. coli was the highest in CA-BSI group, and the incidence of E. coli varied by type of BSI (47.1%, 14.9%, 27.2% in CA-BSI, HA-BSA, and HCA-BSI, respectively, P<0.005). Of CA-BSI isolates, the incidence of Gram-negative aerobes (70.5%) was more than two times higher than that of Gram-positive aerobes (28.2%). E. coli (47.1%) and K. pneumoniae (12.6%) represent more than half of the isolates in CA-BSI followed by S. aureus (7.4%), Streptococcus viridans group (5.0%). Of HA-BSI isolates, 49.1% were Gram-negative aerobes, and 48.0% were Gram-positive aerobes. The most common isolate of HA-BSI was S. aureus (15.2%) followed by coagulase-negative Staphylococcus (15.1%), and E. coli (14.9%). The pattern of isolates in HCA-BSI was more similar to that in CA-BSI than that in HA-BSI. Of HCA-BSI isolates, Gram-negative aerobes (65.5%) were more common than Gram-positive aerobes (34.0%) like CA-BSI. However, isolate distributions of CA-BSI and HCA-BSI group were not identical. While E. coli (47.1% vs. 27.2% in CA-BSI vs. HCA-BSI, P<0.001) and Streptococcus pneumoniae (3.9% vs. 1.0% in CA-BSI vs. HCA-BSI, P=0.04) were recovered more frequently in CA-BSI, S. aureus (7.4% vs. 14.1% in CA-BSI vs. HCA-BSI, P=0.009) and P. aeruginosa (2.9% vs. 7.8% in CA-BSI vs. HCA-BSI, P=0.007) were more prevalent in HCA-BSI.
With regard to resistant pathogens, extended spectrum beta-lactamase (ESBL)-producing E. coli was most frequently recovered in patients with HA-BSI (31.3%), followed by HCA-BSI (14.2%) and CA-BSI (3.3%) (HA-BSI vs. CA-BSI, P<0.001; HA-BSI vs. HCA-BSI, P=0.021; HCA-BSI vs. CA-BSI, P=0.002). ESBL-producing K. pneumoniae was common in patients with HA-BSI (18.9%), followed by HCA-BSI (14.7%) and CA-BSI (4.1%). Although, it did not show the statistical difference for the prevalence of ESBL-producing K. pneumoniae (HA-BSI vs HCA-BSI, P=0.593; HCA-BSI vs. CA-BSI, P=0.092) except between HA-BSI and CA-BSI (P=0.018). Methicillin-resistant Staphylococcus aureus (MRSA) was higher in HA-BSI (69.4%), compared with HCA-BSI (31.0%, P<0.001) and CA-BSI group (17.8%, P<0.001).
Primary infection
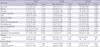
The primary infections causing BSI significantly varied by type of BSI. The most common primary infection of CA-BSI were urinary tract infection (UTI) (31.3%) and intra-abdominal infection (30.5%) (Table 3). In contrast, primary bacteremia (53.2%) was the most common in HA-BSI group followed by intra-abdominal infection (17.6%), and pneumonia (14.2%). The most common primary infection of HCA-BSI was primary bacteremia (39.8%) like HA-BSI, and followed by intra-abdominal infection (27.2%) and UTI (14.2%).
Clinical outcomes
Severity index on admission measured by Pitt bacteremia score in patients with HCA-BSI (2.2±3.0) was significantly higher than that in CA-BSI group (1.5±2.6) (P=0.012) (Table 4). And, the incidence of severe sepsis in HCA-BSI group (36.9%) was also higher than that in CA-BSI (23.4%, P=0.001).
The rate of appropriate empirical antibiotic therapy was the highest in CA-BSI group (89.0%), followed by HCA-BSI (76.4%), and HA-BSI group (75.0%). Initial clinical improvement rate was more frequently observed in CA-BSI group (85.7%) than in HCA-BSI (68.64%, P<0.001) and HA-BSI group (68.5%, P<0.001).
The overall 30-day mortality rate in all patients with BSI was 18% (193/1,144). Mortality rate was significantly lower in CA-BSI group (10.2%) than in HCA-BSI (18.4%, P=0.007), and HA-BSI group (23.0%, P<0.001). Although, no significant difference was seen in mortality rate between HA-BSI and HCA-BSI group (P=0.188).
Risk factors for mortality
By univariate analysis, high Pitt score (>4), severe sepsis, inappropriate empirical antibiotic therapy were the common risk factors for all patients with BSI (Table 5). For demographics and comorbidities, old age (≥65 yr), underlying solid tumor, stroke, high alcohol uptake, neutropenia were the significant risk factors for mortality in CA-BSI group. In HA-BSI group, old age (≥65 yr), underlying congestive heart failure, receipt of immunosuppressant, prior antibiotic use, history of transplantation were the significant risk factors. In HCA-BSI group, underlying congestive heart failure was the significant risk factor. For infecting pathogens, E. coli was the negative predictive factor for 30-day mortality in CA-BSI group. Fungal infection was the significant risk factor for mortality in HA-BSI group. For primary infection, pneumonia was the significant risk factor for all patients with BSI.
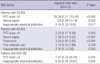
By multivariate analysis, high Pitt score (CA-BSI, OR 28.3, P<0.001; HA-BSI, OR 2.2, P=0.003; HCA-BSI, OR 7.8, P=0.001) and ineffective empirical antibiotic therapy (CA-BSI, OR 5.1, P=0.01; HA-BSI, OR 2.2, P=0.003; HCA-BSI, OR 6.0, P=0.001) were the common independent risk factors in all patients with BSI (Table 6). Severe sepsis (OR 5.5, 95% CI 3.2-9.5, P<0.001), pneumonia (OR 3.0, 95% CI 1.6-5.6, P<0.001), and prior antibiotic use (OR 1.7, 95% CI 1.0-2.9, P=0.03) were the independent risk factors in patients with HA-BSI.
DISCUSSION
This study was a nationwide surveillance of BSI in Korean hospitals. In this study, we compared clinical and microbiological characteristics of 3 types of BSI.
With regard to prevalent pathogens by the epidemiologic type, Gram-negative bacilli (especially E. coli and K. pneumoniae) in CA-BSI were due to higher incidence of UTI and intra-abdominal infection, while Gram-positive cocci (especially staphylococci) in HA-BSI were due to primary bacteremia which were frequently associated with cather-related infection. In HCA-BSI, Gram-negative bacilli were also the prevalent pathogen like CA-BSI, because the incidences of UTI and intra-abdominal infection were higher than that of primary bacteremia. However, the proportion of Gram-negative bacilli in HCA-BSI was differed from that in CA-BSI.
Cheong et al. (16) previously reported that the prevalence of ESBL-producing E.coli in HCA-BSI (6.7%) was higher than that in CA-BSI (3.2%), although it did not show the statistical difference between 2 groups. In addition, Kang et al. (17) reported that more than half (63.2%) of community-onset BSIs caused by ESBL-producing E. coli were HCA-BSI. Our study also showed the similar result that the prevalence of ESBL-producing E. coli in HCA-BSI and HA-BSI group was higher than that in CA-BSI. With regard to S. aureus bacteremia, previous reports showed that the prevalence of MRSA was the highest in in HA-BSI (33.8-61%) followed by HCA-BSI (29.4-52%) and CA-BSI (11-21.2%) (3, 10, 18). And, our study also showed the similar result.
In general, early and appropriate antibiotic therapy significantly affects the overall mortality in BSI (19, 20). Previous studies reported that 10-40% of BSI cases received inappropriate empirical therapy, which was more frequent in cases of HA-BSI and HCA-BSI (9, 21, 22). Our data was also consistent with this finding that initial antibiotic therapy was more frequently inappropriate in HA-BSI and HCA-BSI cases than in CA-BSI. Given the different pathogens and antimicrobial resistance in HCA-BSI compared with CA-BSI, empirical antibiotic choice should be different in HCA-BSI from those in CA-BSI cases.
Previously, high severity index on admission and inappropriate empirical antibiotic therapy were known as significant risk factors in BSI (16, 19, 23). Pazos et al. (23) reported that septic shock, and inappropriate antibiotic therapy were found to be risk factors for mortality in overall BSI. And, Cheong et al. (16) also reported that high Charlson's index, high Pitt score, and acute renal failure were found to be risk factors for mortality in E. coli bacteremia. In our study, high Pitt score and inappropriate empirical antibiotic therapy were shown to be the common independent risk factors in every BSI group including HCA-BSI on multivariate analysis.
There is a limitation in this study. Our data were obtained from a few university hospitals that might lead to the bias of pathogen distribution, antimicrobial resistance or primary infection.
In conclusion, the present data suggest that clinical features, clinical outcome, and microbiologic features of causative pathogens vary by epidemiologic type of BSI. Especially, HCA-BSI shows a distinct entity of BSI with its unique epidemiology, microbiology, and treatment outcomes, which shares more similarity with HA-BSI. The only independent risk factors for mortality associated with HCA-BSI could not be found. However, considering the inappropriate empirical antibiotic therapy as a major independent risk factor for mortality, clinicians should be aware of this category for more appropriate antibiotics based on possible resistant pathogens.


 XML Download
XML Download