

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The septum pellucidum is a thin, membranous midline structure, with two leaves of both white and gray matter, which separates the lateral ventricles. From its superior and anterior aspects, it attaches to the corpus callosum, and from the inferior and posterior aspects, it attaches to the superior part of the fornix body.
The septum pellucidum is partly or completely absent in 2 or 3 individuals per 100,000 in the general population (1). This phenomenon rarely occurs in isolation, but is usually associated with additional malformations of the brain (2). Radiological findings in the absence of the septum pellucidum have included a square or box-like appearance of the frontal horns of the lateral ventricles and an abnormally low position of the fornix from the coronal view. Normally, the inferior border of the septum pellucidum is attached to the upper face of the fornix body; hence the abnormally low position of the fornix in the absence of the septum pellucidum is likely caused of the absence of the tethering effect of the septum pellucidum (2, 3). Therefore, the displaced fornix may lodge in the foramina of Monro and cause intermittent obstruction, resulting in obstructive hydrocephalus.
We report here on two autopsies showing partial absence of the septum pellucidum associated with dilated lateral ventricles and a single midline fornical nodule obstructing the foramina of Monro.
CASE REPORTS
Case 1
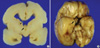
Pregnancy in a 27-yr-old woman was terminated at 36 weeks of gestation after ultrasonography revealed Potter's syndrome in the fetus. The female fetus weighed 1,500 gm and measured 29 cm in crown-rump length and 43 cm in crown-heel length. The head circumference was 26 cm, chest circumference 24 cm and abdominal circumference 20.2 cm. She showed features typical of Potter's syndrome: agenesis of the left kidney with cystic dysplasia of the right kidney, calcaneovarus, pulmonary hypoplasia and exaggerated facial creases. Spina bifida with myeloschisis was present in the lumbosacral area. The brain weighed 294 gm and revealed no abnormalities of gyration, sulcation or cranial nerves. The brain base showed well developed optic chiasma and optic nerves. The optic nerve measured 2.5 mm in diameter. After coronal sectioning, the cerebral hemispheres showed mildly distended lateral ventricles. The corpus callosum was well preserved, which measured 3.0 mm and 1.0 mm in thickness in genu and body, respectively. The anterior commissure appeared normal. The septum pellucidum was absent in its posterior portion. Both fornices was fused to form a single midline nodule, which was inferiorly displaced (Fig. 1). The foramina of Monro were occluded by this round fornical nodule of an abnormally low position. The hippocampus was well formed and fimbria was also present in its usual position and size. The third and fourth ventricles were not dilated. Microscopically, there was no evidence of malformations of cerebral cortical development. Chromosomal analysis of the peripheral blood revealed 46, XX. Maternal serum and urinary estriol and fetal pituitary hormones were not studied.
Case 2
A male fetus was terminated to a 32-yr-old woman at 25 weeks of gestation because prenatal ultrasound showed dilatation of both lateral ventricles and prominent cisterna magna. Dandy-Walker variant and partial agenesis of the corpus callosum were ultrasonographically suspected. The fetus weighed 900 gm and measured 22 cm in crown-rump length and 35 cm in crown-heel length. The head circumference was 25 cm, chest circumference 20.5 cm and abdominal circumference 20 cm. The brain weighed 153 gm and showed no cyst on posterior fossa. Specifically the vermis structure of the cerebellum was normal. Mildly distended lateral ventricle and a well preserved corpus callosum were evident on coronal sections. The septum pellucidum was absent in its posterior portion. Wisps of the septum pellucidum were seen in the anterior portion. A single midline fornical nodule was caudally displaced and jammed into the foramina of Monro (Fig. 2A). The third and fourth ventricles were not dilated and there was no aqueductal stenosis. The brain base was unremarkable with well developed optic chiasma and optic nerves. The optic nerve measured 1.5 mm in diameter (Fig. 2B). Microscopically, there was no evidence of malformations of cerebral cortical development. Maternal serum and urinary estriol and fetal pituitary hormones were not checked.
DISCUSSION
Absence of the septum pellucidum is a congenital defect in the development of the midline telencephalic structures, although it can rarely be an acquired phenomenon, as seen in cases of prolonged, severe hydrocephalus or head trauma (3). Barkovich and Norman reviewed the magnetic resonance images of 35 brains that lacked the septum pellucidum and reported the presence of one or more additional malformations, including septo-optic dysplasia, schizencephaly, Chiari ll malformation, holoprosencephaly, encephalocele, agenesis of the corpus callosum, porencephaly, hydranencephaly and hydrocephalus with aqueductal stenosis, in every case. They used an algorithm to facilitate diagnosis of underlying brain anomaly in patients with absence of the septum pellucidum. But in that algorithm, small optic nerves were not considered a diagnostic criterion for septo-optic dysplasia, which should be differentiated from isolated absence of the septum pellucidum (2). Therefore, it is possible that they might put isolated cases of septal agenesis into septo-optic dysplasia.
Septo-optic dysplasia is a rare congenital disorder characterized by the absence of the septum pellucidum, hypoplasia of the optic nerves, and various types of hypothalamic-pituitary dysfunction (4). Its clinical presentation includes decreased visual acuity, deficiency of growth hormone and antidiuretic hormones, leading to growth delay and diabetes insipidus, low level of thyroid-stimulating hormone, luteinizing hormone and follicular stimulating hormone and mental retardation/developmental delay. The endocrinological deficiencies are found only in 50-90% of cases of septo-optic dysplasia (5, 6) and magnetic resonance images cannot assess precisely the optic nerves and the pituitary gland in utero (7). Therefore, it is difficult to completely rule out septo-optic dysplasia prenatally, even though normal fetal pituitary function and normal appearance of the optic nerves on fetal magnetic resonance images (8, 9). Furthermore, endocrine deficiencies and decreased visual acuity could develop in later life, and those cases should be classified as septo-optic dysplasia. The prevalence of the isolated septal agenesis is practically impossible to know.
In our two cases, septo-optic dysplasia was not considered as a prenatal differential diagnosis because we could not diagnose the absence of the septum pellucidum at prenatal ultrasound. Low maternal estriol in pregnancy is known to be associated with fetal hypopituitarism with ACTH deficiency (10), but we did not check maternal serum and urinary estriol levels as well as fetal pituitary hormones. Although the remote possibility of septo-optic dysplasia remains to be left, well developed optic chiasma and optic nerves without associated brain anomalies favor isolated septal agenesis in the present cases.
Koo et al. (11) reported a case of congenital hydrocephalus associated with complex anomalies of midline telencephalic structures, including absence of the septum pellucidum, hypoplasia of the posterior portion of the corpus callosum, fornical malformation and the hypoplastic hippocampi. The anomalies in our subjects resembled those reported by Koo et al., but were much less severe. The anterior commissure and the corpus callosum were well developed, and the principal anomalies were confined to the septum pellucidum and the fornix.
In the absence of the septum pellucidum, the frontal horns of lateral ventricles consistently assume a square or box-like appearance, and the fornix is displaced caudally (2, 3, 8). Our two cases showed mild ventriculomegaly of the lateral ventricles with blunt angles, which corresponds to a square or box-like appearance on ultrasonographic, computed tomographic and magnetic resonance images of in the absence of the septum pellucidum (2, 3, 8). The clinical significance of the mild ventriculomegaly is uncertain; it may represent a congenital obstructive hydrocephalus or just one of the diagnostic features of the absence of the septum pellucidum.
The fornix is a C-shaped bundle of fibers in the brain that carries signals from the hippocampus to the mammillary bodies and septal nuclei. The inferior margin of the septum pellucidum is attached to the upper face of the fornix body (2, 3). The septum pellucidum, particularly its posterior part is a critical structure to suspend the fornix in proper position and also separation of body of fornix into two parts. In our subjects, the fornices were fused into a single midline nodule and forced into the foramina of Monro, proving the failure of tethering effect of the septum pellucidum.
The foramina of Monro are channels that connect the paired lateral ventricles with the third ventricle. The midline structures above the foramina of Monro include the corpus callosum, septum pellucidum, cavum septum pellucidum, and fornix. In fact, any lesion that obstructs the foramina of Monro can cause hydrocephalus of the lateral ventricle, sparing the third ventricle. We think that the midline fornical nodule formed in the absence of the septum pellucidum, as reported here, may act like a lid on the foramina of Monro and cause intermittent or continuous obstruction. If transient and incomplete, the obstruction would probably not cause hydrocephalus to progress. However, with the fornical nodule forced irreversibly into the foramina of Monro, we can expect progressive, congenital, obstructive hydrocephalus.

 XML Download
XML Download