

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Posttransplant lymphoproliferative disorder (PTLD) is one of the most serious complications after solid organ transplantation and hematopoietic stem cell transplantation (HSCT). The incidence has been reported to be about 1 percent of all transplantations (1, 2). PTLDs, including polyclonal lymphoproliferation of B lymphocytes, polymorphic PTLD and monomorphic B-cell lymphoma, are extremely heterogeneous.
The risk factors for PTLD include the Epstein-Barr virus (EBV) serostatus, primary EBV infection, type of organ transplant, intensity of immunosuppression, presence of cytomegalovirus disease, and age (3-6). EBV infection is thought to play the most important role in the pathogenesis of PTLD (7). During primary EBV infection, EBV infects, transforms and immortalizes host B lymphocytes, and the individual becomes a permanent carrier. EBV-infected B lymphocytes commonly remain in the latent state, protected from viral proteins by preventing death by apoptosis and from causing proliferation. In immunocompetent hosts, the proliferation of B lymphocytes is inhibited by cytotoxic T cells. However, in organ transplant recipients, T-cell function is inhibited through the use of immunosuppressants. Therefore, EBV induces uncontrolled B-cell expansion, resulting in PTLD. In other words, deficiencies of EBV-specific T-cell-mediated immunity may cause PTLD (7-12).
PTLD is successfully treated by reducing immunosuppression. Other treatment methods such as chemotherapy, radiation therapy, antiviral therapy, anti-B-cell monoclonal antibody, and cytotoxic T cells are currently being investigated.
CASE REPORT
A 16-yr-old Korean girl who was previously healthy developed jaundice in March 2005. It progressed to acute fulminant hepatitis 1 month later. A diagnosis of Wilson disease was made on the basis of increased copper in 24-hr urine and a Kayser-Fleischer ring on cornea examination. In April 2005, she received cadaveric liver transplantation. Before transfusion, IgG antibody against viral capsid antigen (VCA) and IgG antibody against Epstein-Barr nuclear antigen (EBNA) were positive, and early antigen (EA) was negative. After liver transplantation, IgG antibody against EA converted to being positive.
Before liver transplantation, there was no cytopenia in blood tests. However, pancytopenia developed after liver transplantation. Absolute neutrophil counts were below 200/µL, which was compatible with severe aplastic anemia. In September 2005, immunotherapy with antilymphocyte globulin (ALG), methylprednisolone and cyclosporine was performed to treat aplastic anemia, but it produced little therapeutic effect.
In January 2006, she received a bone marrow transplant from an unrelated 39-yr-old Korean man who had 4 HLA Ag mismatch (CD34: 1.69×106/kg). The conditioning regimen consisted of fludarabine, antithymocyte globulin (ATG) and cyclophosphamide. ATG depleted T lymphocytes. After transplantation, immunosuppressive induction was performed with cyclosporine but engraftment was failed.
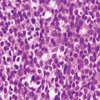
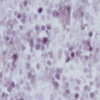
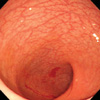
Eleven months after liver transplantation, hematochezia developed. We performed computed tomography (CT) of the abdomen and colonoscopy in order to find the cause of hematochezia. Abdomen CT revealed lymph node enlargement in the mesentery and paraaortic area (Fig. 1). Multiple aphthoid ulcers were found during colonoscopy (Fig. 2). Colon biopsy showed monoclonal B-cell proliferation, which was compatible with polymorphic PTLD (Fig. 3). Positive results for EBV in situ hybridization (Fig. 4) and immunoglobulin heavy chain gene rearrangement were obtained. In addition, EBV DNA was detected by the polymerase chain reaction (PCR) (130.1copies per reaction).
Immunosuppression was reduced for the treatment of PTLD. Cyclosporine was stopped, and prednisolone (10 mg per day) was started. However, 12 months after liver transplantation, colon biopsy still showed monomorphic PTLD and a positive result for EBV in situ hybridization in succession.
Pancytopenia progressed because of engraftment failure. Fourteen months after liver transplantation (June 2006), she received peripheral blood stem cell transplantation again from a 41-yr-old Taiwanese man who had 1 HLA Ag mismatch (CD34: 3.80×106/kg, CD3: 9.224×107/kg). The donor had positive results for EBV and CMV serologic tests. A combination of cyclophosphamide, ATG and TLI served as the conditioning regimen. After transplantation, immunosuppressive induction was achieved with cyclosporine. She suffered from diffuse alveolar hemorrhage, CMV antigenemia and hemorrhagic cystitis. There was no evidence of graft-versus-host disease (GVHD).
One month after the second HSCT, complete DNA chimerism was achieved, and the result of XX/XY FISH was 0.3%/99.7%. In addition, abdomen CT revealed that the size of intra-abdominal lymph nodes markedly decreased (Fig. 5). Colonoscopy revealed that multiple ulcers in the sigmoid colon disappeared (Fig. 6). Blind colon biopsy showed non-specific inflammation. The level of EBV DNA was reduced to 68.65 copies per reaction.
Twenty months after HSCT, she is still alive under immunosuppression with cyclosporine, and there were no lymph node enlargement on abdomen CT scans.
DISCUSSION
To treat PTLD, various treatment strategies including chemotherapy, radiation therapy, antiviral therapy, anti-B-cell monoclonal antibody therapy and modalities for the restoration of EBV-specific cellular immunity, have been employed. Reduction of immunosuppression remains the first-line treatment, and many cases of polyclonal PTLD resolved completely in this manner. However, this was not the case for monoclonal PTLD. Thus, many other therapeutic trials have been attempted.
In this case, the patient underwent liver transplantation due to fulminant hepatitis and also underwent HSCT due to aplastic anemia. PTLD developed 11 months after liver transplantation. Immunosuppression reduction was ineffective in the treatment of PTLD. Recently several studies have supported the role of rituximab as a second-line therapy for PTLD (13-15). However, Rituximab was not administered to the patient because she had severe pancytopenia due to graft failure. A second HSCT can be effective in the treatment of PTLD. We hypothesized that HSCT of an unrelated donor, which contains cytotoxic T lymphocytes presensitized to EBV, might be an effective treatment method. The patient underwent a second HSCT from an unrelated donor, and the lesion of PTLD disappeared.
As mentioned earlier, deficiencies of EBV-specific T-cell-mediated immunity may cause PTLD. Therefore, treatment with EBV-specific cytotoxic T lymphocytes had been tried. Recent reports have documented the benefit of cellular therapy with EBV-specific cytotoxic T lymphocytes (16-20). Cytotoxic T lymphocytes from the blood of a donor are transfused into a recipient with PTLD. In this manner, remission of PTLD has been achieved in as many as 90 percent of patients. In this case, peripheral stem cells, which the patient received at the second HSCT, contain T lymphocytes (CD3: 9.224×107/kg). The amount of T lymphocytes is larger than that of donor leukocyte infusion from a previous study (16). A second HSCT may serve as cellular therapy with cytotoxic T lymphocytes for PTLD.
In this case, we have shown that HSCT can treat PTLD and long-term survival is possible. The mechanism for this is unclear, but it is thought that HSCT serves as cellular therapy with cytotoxic T lymphocytes. Further investigations are needed to identify whether HSCT is an available cellular therapy for refractory PTLD.



 XML Download
XML Download