

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Liver fibrosis represents the wound healing response to chronic liver injury brought about by processes such as chronic viral hepatitis, excessive alcohol consumption, nonalcoholic steatohepatitis, hemochromatosis, or immune-mediated liver injury (1). Cirrhosis develops if liver fibrosis progresses. Cirrhosis is characterized by the presence of bands of fibrosis, parenchymal nodules, and vascular distortion, all of which lead to hepatic dysfunction and the major life-threatening complications that characterize the condition.
Therefore, an accurate assessment of disease severity is important in predicting prognosis and guiding treatment decisions in patients with chronic liver disease. Liver biopsy is still considered the gold standard for assessing liver fibrosis (2). This procedure is very useful because it provides information about the degree of liver fibrosis, as well as the severity and extent of inflammation (2). However, it is invasive and can lead to grave complications (3, 4). Furthermore, its accuracy in assessing fibrosis is questionable because of sampling errors (5-9) and intra- and inter-observer discrepancies (9-11). In addition, because liver biopsy is a static examination, it does not represent the dynamic changes during the progression of liver fibrosis.
To circumvent the limitations of liver biopsy, noninvasive markers have attracted the attention of many investigators, and various markers in the blood have been proposed as potential indicators of liver fibrosis. Some studies have suggested the fibrosis-predicting models composed of several potential blood markers, including AAR (AST/ALT ratio) (12-14), PGA (prothrombin time, γ-GT, apolipoprotein A1), PGAA index (prothrombin time, γ-GT, apolipoprotein A1, α2-macroglobulin), FibroTest® (15), Forns fibrosis index (FFI) (16), and age to platelet ratio index (APRI) (17). Other reports have suggested several serum markers, including collagen, hyaluronic acid, YKL-40, matrix metalloproteinase (MMP), and tissue inhibitor of metalloproteinase (TIMP), all of which have a potential role in the accumulation or degradation of extracellular matrix (ECM) (18, 19). However, comprehensive validating studies dealing with all these blood markers simultaneously in a large group of patients have rarely been carried out, particularly in the area where hepatitis B virus is endemic.
This study was performed prospectively in order to assess and compare the predictive power of a variety of previously-reported surrogate markers for identifying significant fibrosis, and preferably, to establish a more reliable predictive model for liver fibrosis.
MATERIALS AND METHODS
Patients
All consecutive patients with chronic liver disease seen in our institution between June 2006 and December 2007 with an indication for percutaneous liver biopsy were included in this study. Liver biopsy was performed for assessment of the severity of liver fibrosis and inflammation prior to treatment or for the evaluation of the cause of liver disease.
The cause of chronic liver disease was determined using standard diagnostic criteria. Chronic hepatitis B was diagnosed by positive serologic tests for serum hepatitis B surface antigen for at least 6 months. Chronic hepatitis C was diagnosed by serologic detection of hepatitis C antibody and positive serum hepatitis C virus RNA by polymerase chain reaction. Alcoholic liver disease was diagnosed in patients with consumption of at least 80 g of alcohol daily for more than five years without other causes of chronic liver diseases. The diagnosis of nonalcoholic fatty liver disease was in patients with elevated aminotransferses and liver histology showing steatosis in at least 10% of hepatocytes without causes of chronic liver diseases. Primary biliary cirrhosis was diagnosed by at least two of the following criteria: serum alkaline phosphatase more than 1.5 times the upper limit of normal, positive antimitochondrial antibody, and compatible liver histology. The diagnosis of autoimmune hepatitis was based on the revised descriptive criteria reported by the International Autoimmune Hepatitis Group. Patients were excluded from the study if they had any disorder associated with extrahepatic fibrosis, including rheumatic, renal, or lung disease; any cardiovascular disease or cancer; or advanced cirrhosis with evidence of decompensation. Weight and height on the liver biopsy day and average alcohol consumption during the 5 preceding years were recorded for each patient.
All patients provided written informed consent for their participation in the study, and the conditions of the consent were in strict adherence to the principles of the Declaration of Helsinki.
Surrogate markers for fibrosis
Laboratory tests, including platelet count, prothrombin time, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and γ-glutamyl-transpeptidase (γ-GT), were evaluated in all patients on the liver biopsy day, using commercially available assays. Apolipoprotein A1 (Roche, Munich, Germany), α2-macroglobulin (Dade Behring, Marburg, Germany), haptoglobin (Roche, Munich, Germany), collagen IV (Fine chemical, Tokyo, Japan), and hyaluronic acid (Corgenix, Denver, CO, USA) were determined in serum samples using an enzyme immunoassay. The procollagen III N-terminal peptide (PIIINP) concentration was measured using a radioimmunoassay (Orion Diagnostica, Espoo, Finland). A sandwich immunoassay was used to quantify serum YKL-40 (Metra Biosystems/Quidel, San Diego, CA, USA), matrix metalloproteinases (MMP)-2 and -9 (R & D Systems, Minneapolis, MN, USA), and tissue inhibitor of metalloproteinase (TIMP)-1 (R & D Systems). In addition, using the results of surrogate markers, various well-known predictive models for fibrosis, including the AST/ALT ratio (AAR) (20), PGA index (prothrombin time, γ-GT, apolipoprotein A1) (21), PGAA index (prothrombin time, γ-GT, apolipoprotein A1, α2-macroglobulin) (1), Forns fibrosis index (FFI; platelet count, γ-GT, age, cholesterol) (16), AST to platelet ratio index (APRI) (17), age platelet index (API) (22), and cirrhosis discriminant score (CDS; platelet count, AST, ALT, PT INR) (23), were calculated using the equations in Table 1.
Liver histology
Liver biopsies were carried out by ultrasound-guided technique using a 16-gauge biopsy needle, and the total length of the biopsy specimen was more than 1.5 cm. Liver biopsy sections were formalin-fixed, paraffin-embedded, and stained routinely with hematoxylin-eosin-saffron and Masson's trichrome. All liver biopsies were evaluated blindly, and the histological changes of chronic hepatitis were classified according to the Batts and Ludwig scoring system (24) by a single experienced pathologist blinded to both clinical data and the results of noninvasive tests. Fibrosis was staged on a 0-4 scale as follows: F0, no fibrosis; F1, fibrous portal expansion; F2, periportal fibrosis with periportal or rare portal-portal septa; F3, fibrous septa with architectural distortion but no obvious cirrhosis; F4, cirrhosis. Fibrosis was considered significant when the fibrosis stage was F2 or more.
Statistical analysis
All data were analyzed using SPSS statistical package software version 13.0 (SPSS Inc., Chicago, IL, USA). Data are presented as mean±SD. Student t-test and the chi-square test were used to compare quantitative and qualitative variables, respectively. Patients were categorized according to the severity of their histologic lesions. The relationship between fibrosis stage and other variables was assessed using Spearman's correlation analysis. Logistic regression analysis with a stepwise forward approach was used to determine independent predictive markers for significant fibrosis among the various markers. In addition, a new predictive model was constructed by modeling the values of the independent variables and their coefficients of regression. The predictive accuracy was assessed by calculating the area under the receiver-operating characteristics curve (AUROC). AUROCs were compared using the method of Hanley and McNeil (25). A twotailed P value less than 0.05 was considered statistically significant.
RESULTS
Patient characteristics
One hundred fifty-eight patients with chronic liver disease were enrolled in this study. Their demographic and baseline characteristics are summarized in Table 2. There were 111 men and 47 women, and their mean age was 41±13 yr. Causes of chronic liver disease included chronic hepatitis B in 107 patients (67.7%), chronic hepatitis C in 26 (16.5%), nonalcoholic fatty liver disease in 15 (9.5%), alcoholic liver disease in 3 (1.9%), autoimmune hepatitis in 3 (1.9%), primary biliary cirrhosis in 2 (1.3%), and cryptogenic cirrhosis in 2 (1.3%). The fibrosis stages identified on liver biopsy was F0 in 18 patients (11.4%), F1 in 34 (21.5%), F2 in 41 (25.9%), F3 in 41 (25.9%), and F4 in 24 (15.2%). A total of 106 patients (67.1%) had significant fibrosis (≥F2).
Correlations between surrogate markers and stage of liver fibrosis
The results of various markers according to fibrosis stage are presented in Fig. 1, and the correlation between various clinical variables and fibrosis stage are shown in Table 3. Platelet count, prothrombin time, and haptoglobin and MMP-9 levels showed a negative correlation with fibrosis stage (P<0.01), whereas the levels of procollagen III, collagen IV, hyaluronic acid, α2-macroglobulin, MMP-2, TIMP-1, and YKL-40 showed a positive correlation (P<0.01).
The efficacy of various surrogate markers for predicting significant liver fibrosis
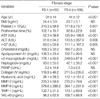
Of 12 single surrogate markers, the AUROCs of hyaluronic acid, haptoglobin, collagen IV, and α2-macroglobulin were above 0.75 (0.81, 0.79, 0.77, and 0.75, respectively) for predicting F≥2 in all enrolled patients. The AUROC of hyaluronic acid was significantly higher than those of platelet count, prothrombin time, PIIINP, MMP-2, MMP-9, TIMP-1, YKL-40, and apolipoprotein A1 (Table 4). Of the previously reported fibrosis prediction models, the AUROCs of the PGAA index, FFI, APRI, and API were above 0.75 (0.75, 0.79, 0.76, and 0.77, respectively) for predicting F≥2. However, the AUROCs of these predictive models were not significantly superior to those of single surrogate markers (Table 4). Subgroup analysis was performed in patients with chronic hepatitis B to exclude the effect of liver disease etiology, and the results were found to be similar to those seen in the whole series (Table 4). Briefly, hyaluronic acid, collagen IV, PGAA, FFI, APRI, and API were useful for the prediction of F≥2 (AUROCs: 0.80, 0.75, 0.81, 0.83, 0.76, and 0.77, respectively).
Uni- and multi-variate analyses for determining factors associated with significant fibrosis (≥F2)
The results of univariate analysis for predicting liver fibrosis stage ≥F2 are represented in Table 5. The markers showing a significant association with fibrosis stages F2-F4 were age (P<0.001); platelet and PT (P<0.05); ALT, AST, and GGT (P<0.01); haptoglobin, MMP-9, hyaluronic acid, α2-macroglobulin, MMP-9, TIMP-1, and YKL-40 (P<0.001). On multivariate analysis, hyaluronic acid, α2-macroglobulin, and haptoglobin were independent predictive factors associated with significant fibrosis (≥F2) (Table 6).
Establishment of a new predictive model for detecting significant fibrosis (F≥2)
In order to establish a predictive model for detecting significant liver fibrosis, the independent predictive factors that were significant on multivariate analysis, including hyaluronic acid, α2-macroglobulin, and haptoglobin, were categorized into three groups according to their values. By providing adequate scores to each category of each factor in consideration of their respective predictive strengths on multivariate analysis, we were able to establish a new predictive model for significant liver fibrosis, the AHH index (Table 7). AHH score is calculated by the sum of the scores of three variables.
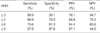
The scores were significantly different between patients with F0-1 (3.2±1.8) and those with F2-4 (6.7±1.8; P<0.001) (Fig. 2). The AUROC for ≥F2 on the AHH index was 0.91 (95% confidence interval [CI], 0.85-0.96; P<0.001), which was significantly higher than that of single serum markers like hyaluronic acid, haptoglobin, collagen IV, and α2-macroglobulin, as well as those of previously-reported fibrosis prediction models like the PGAA index, FFI, APRI, and API. Furthermore, the AHH index also showed relatively good accuracy for predicting ≥F3 and F4 with AUROCs for ≥F3 and F4 of 0.82 (95% CI, 0.75-0.89) and 0.81 (95% CI, 0.73-0.89), respectively. Predictive efficacies of the AHH index for detecting significant liver fibrosis (≥F2) with various cutoff values are shown in Table 8. Using the cutoff value of 5, the AHH index demonstrated an 89% sensitivity, 78% specificity, 89% positive predictive value, and 78% negative predictive value in predicting ≥F2. The ROC curve of the AHH index is presented in Fig. 3.
DISCUSSION
In the management of chronic liver disease, it is clinically important to assess the progression of liver fibrosis. Furthermore, with recent improvements in treatment modalities for chronic liver disease, there is an increasing need for accurate noninvasive methods, such as surrogate blood markers, which enable repetitive measurement of the degree of liver fibrosis. In order for these blood markers to be utilized as accurate predictors of the degree of liver fibrosis, 1) they should reflect the specific changes in the liver during the progression of fibrosis, 2) they should be sensitive both to fibrogenesis and fibrolysis, 3) their metabolic pathways should be defined, and their blood levels and half-life should not be influenced by the function of the liver, kidney, or reticuloendothelial system, and 4) they should be easily measured. However, it is not easy to find a marker that fulfills all these criteria (18, 19).
Liver fibrosis results from accumulation of ECM as a consequence of chronic liver injury, leading to architectural changes in the liver parenchyma that eventually cause liver dysfunction and portal hypertension. Therefore, both direct markers, such as components of ECM itself or factors that are involved in the synthesis or degradation of ECM, and indirect markers influenced by liver injury, altered liver function, or portal hypertension are all potential markers for predicting the stages of liver fibrosis. For examples, as indirect markers, AST, ALT, and γ-GT reflect liver injury; prothrombin time, cholesterol, haptoglobin, and α2-macroglobulin reflect altered liver function caused by architectural changes; platelet counts are closely related with portal hypertension. Collagen, glycoprotein, and proteoglycan, which are components of the ECM, have drawn attention as potential direct markers. Accumulation of these ECM components could be caused not only by an increase in their synthesis, but also by a decrease in their degradation, which might be caused by over-stimulation of the expression of tissue inhibitor of metalloproteinase (26, 27).
Most studies related to blood markers predicting liver fibrosis have been performed in Western patients with chronic hepatitis C, and it is unknown if their findings can be applied directly to the Asian people. Furthermore, most previous studies have focused on 1 or 2 potential markers predictive of liver fibrosis. Thus, few large comparative studies investigating the majority of these direct and indirect fibrosis markers have been performed. In this study, we included most previouslyknown direct or indirect potential markers of liver fibrosis and tried to determine if they could also be used in Korean patients, in whom chronic hepatitis B is the main cause of chronic liver disease.
We found that various direct and indirect blood markers known as useful predictors of liver fibrosis in previous Western studies were also valuable in Korean patients. In particular, α2-macroglobulin, haptoglobin, and hyaluronic acid were independent factors predictive of significant liver fibrosis on multivariate regression analysis. α2-macroglobulin and haptoglobin, the two major components of α2-globulin, are synthesized in hepatocytes, but α2-macroglobulin is also synthesized in hepatic stellate cells. Generally, α2-macroglobulin is an acute-phase protein, and its synthesis increases with the activation of hepatic stellate cells in inflammatory condition and may precipitate liver fibrosis via its inhibition of collagenase (1). Previous studies have already reported that haptoglobin has a negative correlation with the progression of liver fibrosis independent of hemolysis, hypersplenism, or liver failure (16, 28). It has also been suggested that haptoglobin might be related to the growth factors that vary with the progression of liver fibrosis (16). In the present study, hyaluronic acid showed the highest AUROC for predicting ≥F2 among the various single fibrosis markers studied, and its AUROC was superior to those of pre-existing liver fibrosis prediction models such as PGAA, FFI, APRI, and API. The increase in hyaluronic acid in chronic liver disease is caused by increased synthesis by hepatic stellate cells and by a decrease in uptake and degradation by sinusoidal cells. Our results were consistent with previous reports suggesting the usefulness of hyaluronic acid as a liver fibrosis marker (29, 30).
Finally, we constructed the AHH index for the prediction of significant fibrosis with these three independent predictive markers: α2-macroglobulin, haptoglobin, and hyaluronic acid. The AUROC for predicting ≥F2 of the AHH index was 0.91, which is superior to the AUROCs of the PGA index, PGAA index, FFI, APRI, and API. These results suggest that the AHH index could be a good model for predicting significant fibrosis in Korean patients with chronic liver disease. Further validation studies are needed to evaluate the predictive efficacy of the AHH index.
In conclusion, α2-macroglobulin, haptoglobin, and hyaluronic acid were independent factors for predicting significant liver fibrosis in our patients with chronic liver disease. These markers enabled us to establish a new predictive model useful for detecting significant liver fibrosis.









 XML Download
XML Download