

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hematopoietic stem cell transplantation (HSCT) is currently the treatment of choice for many hematologic malignancies and severe congenital or acquired disorders of hematopoietic or immune system. HSCT recipients are at high risk for a variety of pulmonary complications. Pulmonary complications occur in 25-50% of allogeneic HSCT recipients, and can account for approximately 50% of transplant related death (1). With prolonged survival after HSCT, there is an increased recognition of the relatively late post transplantation syndrome of lymphoid bronchiolitis, bronchiolitis obliterans (BO) or bronchiolitis obliterans organizing pneumonia (BOOP). The latter 2 conditions are known for being the most common causes of thoracic air-leakage syndrome (TALS), which was defined by Franquet et al. for the presence of extra-alveolar air including spontaneous pneumomediastinum, pneumopericardium, subcutaneous emphysema, interstitial emphysema, and spontaneous pneumothorax (2, 3).
Since the first description of TALS by Franquet et al., the incidence or clinical nature, effects on prognosis remains unclear. There are only a few clinical and radiological reports concerning this condition, and in majority of reported cases, TALS seemed to be associated with fatal prognosis (4-6). However, the clinical and temporal course has not been well evaluated. As far as we know, this is the first article reporting large numbers of TALS among more than thousands of HSCT patients. The purpose of this study was to describe the fatal clinical course and significant outcome of patients with TALS following HSCT.
MATERIALS AND METHODS
We retrospectively analyzed 2,177 patients who received BMT at the St. Mary's hospital between from January 2000 to July 2007. The database was searched for patients with the diagnosis of pneumomediastinum, pneumothorax, pneumopericardium, subcutaneous emphysema, interstitial emphysema, and when patients were found, their medical and radiological records were reviewed. Patients with an identifiable other than spontaneous cause of TALS or patients with autologous peripheral blood stem cell transplantation were excluded, leaving 18 cases with spontaneous cause of TALS.
All medical, radiological, and available histopathological records were further reviewed to confirm acute or chronic graft-versus-host disease (GVHD). The diagnosis of acute or chronic GVHD was made by using published criteria for clinical manifestation and histopathological examination of the skin, oral mucosa, esophageal, liver, and bronchial and open lung biopsy samples whenever possible (7-9). The diagnosis of GVHD was determined by either histopathologic (n=9) or clinical (n=9) evidence.
BOOP was defined as organizing pneumonia as secondary reaction in chronic bronchiolitis. CT features regarded as representing BOOP were bilateral, patchy, and asymmetric areas of airspace consolidation with sub-pleural or peribronchovascular distribution as well as patchy and asymmetric ground-glass opacity (10). BO was defined based on clinical, histopathological and CT findings. Areas of decreased attenuation of lung parenchyma, expiratory air trapping and subsegmental or segmental bronchial dilatation, as well as peribronchiolar opacities were regarded as signs of BO on chest CT (2). CT examinations were obtained by using either a single-detector row CT scanner (Somatom Plus 4, Siemens Medical Solutions), or a multi-detector row CT scanner (Volume Zoom, Siemens Medical Solutions, Forchheim, Germanny). Duration of thoracic air-leakage was calculated from the date of occurrence to the date of resolution on chest CT or to the moment of death in case of persistent TALS.
This study was reviewed and approved by the Institutional Review Board of the Catholic University of Korea (approval number: SC09FZZ0105).
RESULTS
Patient characteristics
Of the 2,177 patients undergoing HSCT during the assessed 8.5-yr, total 19 patients developed thoracic air leakage syndrome, and 18 patients could be included in the study. One patient was excluded because he received autologous peripheral blood stem cell transplantation. The overall incidence could be calculated as 0.83% (18/2,177).
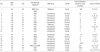
Mean age of the patients was 36.3±12.3 yr old (18-64 yr old). All patients received allogeneic HSCT, four of them were fully matched allogeneic HSCT, however, and others were unmatched at least more than 1 locus of HLA mismatching (Table 1).
No patients had history of previous pneumothorax. Two of them had pulmonary tuberculosis before allogeneic HSCT, and they were cured after the treatment. Current smoker was 1 at the time of allogeneic HSCT, others were non-smokers.
GVHD was diagnosed after allogeneic HSCT at the mean 103.5±135.1 days (21-471 days) after HSCT by clinical, radiological (abdominal ultrasonography, nonenhanced or enhanced chest computed tomography), or pathological (skin biopsy, endoscopic gastrointestinal mucosal biopsy, lung biopsy) method.
Treatment for GVHD continued for all patients including steroid and immunosuppressant, but GVHD progressed in all patients except 2 patients (No. 5 and 7).
Clinical features and outcomes of TALS
The onset of TALS was mean 425.9±417.8 days (60-1,825 days) after HSCT, and the duration was mean 16.3±21 days (2-90 days). The most common feature of TALS was spontaneous pneumothroax (n=14), and followed by subcutaneous emphysema (n=6), pneumomediastinum (n=5), interstitial emphysema (n=2), and pneumopericardium (n=1). More than two types of TALS appeared at the same time at 7 patients (Table 2). In patients with pneumothorax, sidedness were right in nine patients, left in seven patients, concurrent bilateral in one, and sequential bilateral in one patient.
The causes of TALS were spontaneous in 2 survivors and 9 non-survivors. In the other 7 non-survivors, TALS occurred after ventilator appliance due to decreased pulmonary function.
Concurrent radiological finding on chest radiograph at the time of onset of TALS were bilateral atypical patchy consolidation (n=9), atypical pneumonia (n=5), pulmonary edema (n=3), and pleural effusion (n=1).
TALS was treated according to the type of each manifestation, mainly by chest tube and oxygen supply. One patient refused the treatment. The result of treatment was poor; 12 patients recovered from TALS, while other 6 patients suffered from persistent TALS. In 6 patients TALS persisted and died in the same hospitalization period. In 12 patients, only 2 patients could survive. Ten patients recovered from TALS, but 6 patients died during the same hospitalization due to respiratory failure (n=3) and brain hemorrhage (n=1). The reason of respiratory failure were aggravation of GVHD and concurrent pneumonia. The other 4 patients (No. 2, 4, 15, and 16) died at 117-1,046 days after TALS onset due to aggravation of lung GVHD.
DISCUSSION
Chronic GVHD is the most common non-relapse problem in HSCT patients, occurring in approximately 60% to 80% of long term survivors of allogeneic HSC transplant (11). The true incidence of TALS in allogeneic HSCT with GVHD related BO is unknown because of the scarcity of cases reported in the literature. Franquet et al. (12) estimated the incidence in his retrospective review of 9 air leak syndrome cases as 1.05% by using yearly estimated cumulative incidence. Another report about spontaneous thoracic air leak syndrome in allogeneic HSCT, the incidence was 2.3% (6/300 patients) (10). As far as we know, this study was the largest study about TALS. We reviewed 2177 HSCT cases from January 2000 to July 2008, and we found 19 TALS, and the incidence was 0.83%.
There are three characteristics related to TALS. First, TALS was one of clinical manifestations of BO/BOOP as underlying GVHD in patients received HSCT. Second, TALS could not be easily treated by the usual means of treating pneumothorax, pneumomediastinum, or subcutaneous emphysema. Third, TALS can be regarded as indicator suggesting poor prognosis of the patients.
BO/BOOP, a late complication of bone marrow transplantation, is associated with GVHD and is frequently fatal. BO was first described by Roca et al. (13) in 1982 in a patient with chronic GVHD. Since then, several studies have reported a 2% to 20% incidence of BO in HSCT patients (2). By a study of Vogel et al. (10), the incidence of TALS among total HSCT patients was 2.3%, and that among BO/BOOP patients was higher, 20%. BO/BOOP are known for being the most common cause of TALS (4, 10, 14). In this study, all patients had GVHD at the onset of TALS, and 2 were biopsy-proven BO and BOOP, while other 16 patients diagnosed having BO/BOOP by clinical or radiologic studies.
The condition is usually progressive and fatal, as mentioned in other reports (15). Treatment was given according to the type of TALS, but the response was poor; TALS persisted in 6 patients until death (33.3%). TALS resolved in 12 patients, but the duration of TALS was not short, mean 20.7 days (2-90 days) were required for recovery. Persistent air-leak may require pleurodesis or pleurectomy, but in our study, it was impossible because of the fragile condition of the patients (15, 16).
TALS and BO/BOOP, GVHD might be related each other in the development. Pathogenesis of BO in HSCT recipients has not yet been well defined. It has been suggested that the changes leading to the cicatrical form of BO may evolve from interstitial pneumonia and BOOP (17). The cause of obstructive airway disease and BO in transplant recipient is unclear. Postulated causes include viral infection, autoimmunity, and damage to small airways. BO is higher in bone marrow transplant recipients with GVHD than in those without (6% vs. 0%). The same applies for obstructive lung disease. Clinically BO and obstructive pulmonary airway disease are usually manifested symptomatically in the first year after transplantation (14).
In most cases TALS is caused by alveolar rupture, leading initially to pulmonary interstitial emphysema and then traveling centrally along the bronchovascular sheaths into the mediastinum. This pathogenetic mechanism is called the Macklin effect and relates to a three-step pathophysiologic process: blunt traumatic alveolar ruptures, air dissection along bronchovascular sheaths and spreading of this blunt pulmonary interstitial emphysema into the mediastinum (18). In BOOP, localized or regional peripheral obstruction can result in ball-valve effect, distal over distension leading to burst alveoli and entry of air into the bronchovascular sheath, or, in a similar way, to Macklin effect.
However, other possible causes of TALS, such as aspergillosis and Pneumocystis pneumonia, must be excluded (15). The emphysema may result from lung injury, caused by pretransplantation chemotherapy, total-body irradiation, GVHD, immunosuppressant, or infections such as aspergillosis, candidiasis, and Pneumocystis pneumonia (14).
BO/BOOP can cause ALS, but BO/BOOP may often present initially as a recurrent spontaneous pneumothroax and then develop multi-system complications (19). It is noteworthy that three patients (No. 2, 9,15), BO/BOOP was diagnosed at the same time the occurrence of TALS. All of the 3 patients died due to aggravation of GVHD after the resolution of TALS.
TALS probably is not be the direct cause of death in post transplant patients, but it might be an indicator showing worse prognosis and pulmonary complications. The condition is usually fatal. In this study, the patients with TALS showed high mortality as 16 among 18 patients died after the development of TALS (88.9%). In our study, the most common direct cause of death was respiratory failure associated with aggravation of GVHD, and the second was pneumonia. This finding coincides with that in previous literature, reported mortality of BO related with GVHD is 21-100%, and mortality of TALS is 66.7-100% (10, 19, 20).
In conclusion, we suggest that TALS may complicate BO/BOOP or can be an initial manifestation of BO/BOOP. TALS is hard to be resolved, and even after the recovery, patients hardly can survive because of aggravation of GVHD. We suggest specifically in HSCT patients, when once developed, TALS seems hard to be cured, and as a result, can be related to high fatality.

 XML Download
XML Download