

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cerebrospinal fluid (CSF) shunts are a definite treatment for hydrocephalus. As increasing numbers of women have CSF shunts placed to treat hydrocephalus, more shunt-dependent women are becoming pregnant (1, 2). Although the maternal and fetal outcome in patients with ventriculoperitoneal (VP) shunts is uniformly excellent, the changes in the abdominal cavity, such as the enlargement of the uterus and increased abdominal pressure, could cause shunt failure (1, 3-5). The distal shunt catheter is frequently obstructed in pregnancy, especially during the third trimester when the intra-abdominal pressure is thought to be highest (3, 4). Postpartum shunt complications are rare (1, 4, 6, 7), and shunt obstruction immediately after a cesarean section had not been reported. We present a patient with a VP shunt who had reduced consciousness due to obstruction of the abdominal shunt catheter immediately after a cesarean section delivery.
CASE REPORT
A 32-yr-old woman, G2P2A0L2, came to the emergency department complaining that she felt drowsy. She had undergone a cesarean section delivery of a full-term healthy baby (3,200 gm) the day before. At the age of 26 yr, she had a VP shunt placed to treat hydrocephalus associated with meningitis. She underwent a shunt revision when she was 29 yr old. At that time, she was in the sixth month of her first pregnancy and complained of drowsiness and headache. Her husband said that the reason for the shunt malfunction had not been determined and the malfunctioning VP shunt had been replaced with a new device. The revision surgery had successfully relieved her symptoms. At full term, she underwent a lower segment cesarean section because of fetal distress and gave birth to her first child, who weighed 3,580 g. The postpartum course was unremarkable after the birth of her first child.
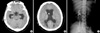
At 31 yr of age, she became pregnant with her second child. She had no symptoms related to shunt malfunction during gestation. A repeated cesarean section was performed at the same private obstetrics clinic and a healthy baby was delivered. The peritoneal cavity was not irrigated and the shunt tube was not observed at surgery. She began to complain of a headache 12 hr after the cesarean section. Her consciousness deteriorated gradually and she became drowsy. She was transferred to our hospital 24 hr postoperatively. In the emergency room, she did not open her eyes spontaneously and her verbal response was very slow and inappropriate. Ventriculomegaly with a bifrontal index of 41% was seen on brain computed tomography (CT, Fig. 1). The shunt catheter was placed properly in her head and abdomen (Fig. 1). When the flushing device was pumped, it was hard to pump. Ten milliters of CSF was aspirated from the flushing device. The aspirated CSF was clear and no laboratory evidence of infection was observed. After aspirating the CSF, her consciousness improved remarkably, and she became alert. Malfunction of the catheter distal to the flushing device was strongly suspected.
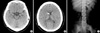
After preparing the skin with alcohol and povidone/iodine solution, a skin incision was made at the previous operative scar in the abdomen. The shunt catheter was placed in the peritoneal cavity and pulled out. The catheter was patent externally, but no CSF was observed dripping from the catheter hole. No CSF flow was observed on pumping the flushing device. When 10 cm was cut from the end of the catheter, CSF dripped steadily from the catheter. The cutoff catheter had been occluded by a blood clot when it was irrigated. The remaining catheter was repositioned in the peritoneal cavity. Her consciousness recovered fully immediately after the operation and her ventricle size returned to normal (Fig. 2).
DISCUSSION
With the development of shunt devices and the increasing success in treating hydrocephalus, more women with CSF shunts are surviving to child-bearing age. Abdominal complications are common with VP shunts (8, 9) and these may increase with the abdominal changes during pregnancy. As a result, a broad range of interdisciplinary health care professionals in neurosurgery and obstetrics will require information about the management of these patients, especially during pregnancy and delivery (1). Interdisciplinary management of pregnant woman with CSF shunts should be performed during the preconception, antepartum, and postpartum periods.
The early preconception management includes an evaluation of medication, especially anticonvulsants, which may be associated with increased risks to fetal development, and image studies to measure the baseline size of the ventricles. During pregnancy in patients with shunts, the patients should be watched for symptoms and signs of increased intracranial pressure (ICP). Signs of increased ICP were reported in 58% of pregnancies with shunts (5). The most common symptoms are headache, nausea, vomiting, drowsiness, gaze paresis, ataxia, and seizures. However, the symptoms of increased ICP are not always associated with shunt malfunction (5, 10-12). Women with well functioning shunts frequently have symptoms of increased ICP during pregnancy because of an increase in brain water and venous distension (10). Therefore, brain images before conception are important for determining whether the shunt is functioning during pregnancy in patients with shunts. If the CSF shunt is functioning inappropriately during pregnancy, the imaging studies show greater enlargement of the ventricles compared to the preconception study. Magnetic resonance imaging seems to be a safe, effective tool for monitoring ventricular dilatation and diagnosing shunt failure (5, 7).
In addition, the pregnancy of a woman with a CSF shunt differs from that of a normal pregnancy, primarily during the third trimester. The flow of CSF in pregnant women decreases either because the shunt is being compressed between the gravid uterus and other internal organs or because the intraabdominal pressure has increased secondary to the large size of the uterus (2). As a ventriculo-atrial (VA) or ventriculopleural (VPL) shunt may be influenced less by the increased abdominal pressure, some studies have advocated that a VA shunt be considered on revision of a VP shunt or during the initial surgery for hydrocephalus in pregnant woman (2, 3, 5, 13, 14). VA or VPL shunts might be preferable to avoid uterine trauma on the placement of a distal catheter. Moreover, shunt revisions in the case of VA shunts have also been reported (1). Endoscopic third ventriculostomy is one treatment modality for pregnant patients with newly diagnosed obstructive hydrocephalus and malfunction of a preexisting shunt (15).
Although a chance of shunt malfunction related to pregnancy has always existed, few cases require shunt revision. Liakos et al. (1) reported that the rates of shunt malfunction and revision before delivery were 13.7% and 5.0%, respectively, in 138 shunt-dependent pregnancies. In their review of the literature, Okagaki et al. (13) found that only 2 (12.5%) of 16 pregnancies with CSF shunts required revision. Many patients with shunt malfunctions can be managed with bed rest and manual pumping of the flushing device of the shunt. In addition, one should remember that the symptoms of increased ICP may mimic those of preeclampsia and an appropriate workup should be obtained (5).
The outcomes of pregnancy in terms of live births are overwhelmingly favorable (1, 3, 16). The mode of delivery should be managed carefully in pregnancies with CSF shunts, and a vaginal delivery is preferred to a cesarean section (1, 2, 4, 5). Vaginal deliveries should be attempted in pregnancies with VP shunts unless cesarean sections are inevitably required for obstetrical or neurosurgical reasons (17). A shortened second stage is preferred to obviate straining and consequent elevation of the ICP. General anesthesia is preferred for the surgical delivery of such patients, while epidural anesthesia is not recommended because an inadvertent dural puncture might result in contamination of the CSF (3, 5).
A cesarean section may cause adhesion formation around the shunt tip in VP shunts and may increase the possibility of shunt infections, as bacteremia occurs more often after cesarean sections (5). Meticulous hemostasis and profuse irrigation of the peritoneal cavity should be performed to minimize the risk of future obstruction due to fibrin deposition on the end of the shunt (3). Fourteen women (10.1%) in 138 shunt-dependent pregnancies had postpartum revisions, of which eight were vaginal deliveries and six were cesarean sections (1). However, no acute shunt failures occurred during the course of delivery in these reports. In our case, the shunt failure developed immediately after cesarean delivery. We believe that the shunt failure resulted from blood sludge spilling into the peritoneal cavity during the cesarean section. Since peritoneal blood spilled during cesarean section may cause shunt obstruction, the obstetric surgeon should clean the peritoneal cavity when a VP shunt exists. Acute obstruction of the distal catheter must be managed as an emergency because it can lead to a significant increase in the intracranial pressure.
Pregnant women with CSF shunts should be managed in a routine fashion and an awareness of CSF shunt failures manifested by the signs of increased intracranial pressure is necessary to create an index of suspicion for the obstetrician. In addition, a neurosurgeon should be consulted during the antepartum, intrapartum, and postpartum periods. We summarize the recommendations for management of shunt malfunction in shunt-dependent pregnancy (Table 1).

 XML Download
XML Download