

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary pancreatic lymphoma (PPL) is defined as an extranodal lymphoma arising in the pancreas with the bulk of the tumor localized to the pancreas (1). PPL is a very rare disease, accounting for less than 0.5% of pancreatic tumors (1). Since PPLs are reported to have a better prognosis compared to carcinomas, and chemotherapy is the mainstay of the treatment, it is crucial to differentiate PPL from pancreatic carcinoma (2).
Most reports on PPL are single case reports. The objectives of this study were to investigate the characteristics of PPL in Korean patients, and to report our experience with this rare disease.
MATERIALS AND METHODS
We retrospectively evaluated four patients who were pathologically diagnosed with PPL from January 1, 1997 to December 31, 2007 at Seoul National University Hospital. The diagnosis of PPL was based on the criteria defined by Dawson et al. (3) (Table 1). The endpoints of this study were death of the patient or June 30, 2008. Gender, age at diagnosis, classification of the lymphoma, cell lineage, presenting symptoms and signs, laboratory results, location of the tumor in the pancreas, characteristics of computed tomography (CT) imaging, involvement of lymph nodes, extrapancreatic organ involvement, stage, treatment, and outcome of the patients were evaluated. The follow-up and survival information were obtained by contacting the Resident Service Division of the Ministry of Public Administration and Security, Seoul, Korea, and by reviewing medical records. All analyses were done using SPSS for Windows Ver. 11.0 (SPSS Inc., Chicago, IL, USA). This study was approved by the institutional review board at our hospital (IRB number 1001-011-305).
RESULTS
Diagnosis, clinical presentation, and laboratory findings
A total of 4 patients were collected (Table 2). Three patients were male. The diagnoses were: diffuse large B cell lymphoma (n=2), Ki-1 (+) anaplastic large cell lymphoma (n=1), and Burkitt lymphoma (n=1). Three cases were of B cell lineage (diffuse large B cell lymphoma and Burkitt lymphoma); one case was of T cell lineage (Ki-1 [+] anaplastic large cell lymphoma) (Fig. 1). The median age at diagnosis was 46.5 yr (range 11-80 yr). All patients presented with abdominal pain; two patients had evidence of pancreatitis. Other symptoms and signs were weight loss (n=2) and a palpable abdominal mass (n=1). No patient presented with fever or night sweats. No patient had evidence of HIV infection; no patient had a history of organ transplantation.
The serum lactate dehydrogenase (LDH) was measured in three patients. One patient had an elevated serum LDH (>225 IU/L). The serum CEA and CA 19-9 were measured in two patients. No patient had an elevated serum CEA or CA 19-9. No patient had an elevated serum bilirubin. All patients underwent ultrasound-guided percutaneous biopsy of the pancreas for tissue acquisition. There were no complications after the biopsy. No patient underwent surgical procedures, either for diagnostic or therapeutic purposes. Two of four patients underwent bone marrow examination; no patient had bone marrow involvement.
Radiological findings and stages
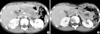
The CT findings are summarized in Table 3. The locations of the lesions were body and tail (n=2), body (n=1), and diffuse involvement of the entire pancreas (n=1). Three patients demonstrated homogenous hypodense pancreatic lesions, and one patient demonstrated a heterogenous hypodense pancreatic lesion. The median long diameter of the mass on CT was 5 cm (range 3-12 cm). Two patients who presented with pancreatitis showed minimal pancreatic duct dilatation on CT, whereas one of the two patients who did not present with pancreatitis showed minimal main pancreatic duct dilatation and the other showed no main pancreatic duct dilatation. One patient showed lymph node enlargement on the same side of the diaphragm. No patient demonstrated lymph node enlargement above the diaphragm. One patient demonstrated extrapancreatic organ involvement in both kidneys (Fig. 2). The Ann Arbor stages of the patients were: IEA (n=1), IIEA (n=1), and IVEB (n=2).
Treatment and prognosis
The patient with stage IEA disease underwent chemotherapy and radiation therapy; this patient had a complete remission after treatment. The patient with stage IVEB disease had chemotherapy; this patient showed relapse in the bone marrow, central nervous system, liver, and the kidneys 6.8 months after the diagnosis. The patient underwent peripheral blood stem cell transplantation and is alive at 30 months. Two patients (stages IVEB and IIEA) refused to be treated and did not have any treatment, and both died 0.8 and 7.0 months after diagnosis, respectively (Table 4).
DISCUSSION
PPL is a rare disease. In a review by Saif in 2006, fewer than 150 cases of PPL have been reported in English literature at that time (4). Most are single case reports. Single center experiences usually have included less than 15 cases (2, 5-11). A nationwide study from Japan reported on 19 cases of PPL (12). In our study, four patients were diagnosed over an 11-yr period. To the best of our knowledge, five cases of primary pancreatic lymphoma have been reported in Korea (13-17).
The clinical presentation of PPL is usually nonspecific. B symptoms (weight loss, fever, and night sweats) are uncommon. Therefore, the clinical presentation will usually help little in distinguishing PPL patients from those with other types of pancreatic tumors (18). Patient with a large, palpable pancreatic mass, presenting with abdominal pain without jaundice, mass homogenous on imaging, with elevated serum LDH may be suspected to have PPL (5, 19). The most common presenting symptom of PPL is abdominal pain, followed by abdominal mass, weight loss, jaundice, acute pancreatitis, small bowel obstruction, and diarrhea (4). In our experience, all patients presented with abdominal pain, and two patients had pancreatitis. No patient developed jaundice in our study. B symptoms other than weight loss (i.e., fever and night sweats) have been reported to be rare in PPL patients. Although weight loss was present in two patients, fever and night sweats were not present in any of our patients.
The head of the pancreas is reported to be the most common location of PPL (2, 7, 12). However, the body/tail region is reported to be more frequently affected in some reports (5). In our study, one of four patients had pancreatic head involvement; this patient showed diffuse involvement of the entire pancreas.
There are reports of PPL arising in the setting of immunodeficiency, such as AIDS or organ transplant (20, 21). In our study, however, no patient had evidence of AIDS or history of organ transplantation.
The majority of PPLs are of the B-cell type (2, 5-7). T-cell PPLs are rare, as described in Japanese series (12). In the Japanese report, although not statistically significant, the 1-yr survival for B-cell PPL (51.9%) was higher than that for T-cell PPL (0%) (12). Among the four patients in our study, only one patient had a T-cell lineage. This patient (initial stage IIEA) did not undergo any treatment, and died seven months after the diagnosis.
There have been controversies over the treatment of PPLs. However, chemotherapy, not surgery, is accepted as the mainstay of the treatment (4, 18). Using complex treatment approaches, cure rates of over 30% of PPL patients by chemotherapy was reported as early as the 1980s (22). With advances in chemotherapy such as monoclonal antibodies, complete remission can be expected in up to 85% of patients with diffuse large B cell lymphoma (23). It is advocated that surgery should be reserved for cases where percutaneous or endoscopic biopsies are not diagnostic, or treatment with chemotherapy and/or radiation therapy is not successful (4, 18). In our study, no patient underwent surgical procedures. The stage IEA patient, who underwent chemotherapy and radiation therapy, achieved a long-term complete remission. The other treated patient, who had stage IVEB disease, relapsed after initial treatment. After subsequent treatment, this patient is alive at 30 months. The treated patients are alive without evidence of disease for more than two years.
In conclusion, PPL is a rare disease. Since chemotherapy is the mainstay of the treatment, differentiation from other pancreatic malignancies is crucial. Nonsurgical biopsy modalities appear adequate for the diagnosis of PPL. Chemotherapy-based treatment, and addition of radiation therapy, if possible, may provide a good prognosis.





 XML Download
XML Download