

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Fever, defined as an increase in body temperature above 38.3℃ (100.4°F), occurs in approximately one-third of all medical patients during their hospital stay (1). Intensive care unit (ICU) patients frequently develop fevers which can originate from infectious or non-infectious causes (2-4). The main causes of non-infectious fever include myocardial infarction, pulmonary embolism, deep vein thrombosis, cerebral infarction, hemorrhage, atelectasis, pancreatitis, acalculus cholecystitis, drug fever, and postoperative fever. On the other hand, major causes of infectious fever in the ICU include ventilator-associated pneumonia, sinusitis, catheter-related infections, nosocomial diarrhea, and wound infections (5).
Fever has multiple clinical effects: increased energy expenditure, myocardial, and respiratory demands, as well as discomfort and worse central nervous system (CNS) injury. On the other hand, fever is regarded as a beneficial host immune response to infection (6). Fever frequently leads to a series of diagnostic work-ups which significantly increase medical costs and expose the patient to the risk of invasive procedures. Empirical treatment of fever, which frequently follows diagnostic work-ups, may result in the inappropriate use of antibiotics and an increase in antibiotic- resistant pathogens. As such, early and accurate differentiation between infectious and non-infectious fever is very important.
Several biologic markers have been tested for their ability to discriminate between infectious and noninfectious fever, including serum procalcitonin (PCT), C-reactive protein (CRP), tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) (7). However, none of these markers have been proven to have enough power to be useful in clinical practice.
The high mobility group box-1 (HMGB1) protein is a 30 kDa nonhistone nuclear DNA binding protein that has been shown to have an extracellular role in inflammation, cell differentiation, adherence, and motility (8). HMGB1 has also been proposed as one of the mediators of sepsis (9, 10). Therefore, HMGB1 may be useful as a differential marker for the evaluation of fever in ICU patients (11). However, serum HMGB1 has not yet been evaluated for this purpose.
Febrile patients by infectious cause of fever have more chance to develop organ dysfunction and subsequent high score in acute physiology and chronic health evaluation (APACHE) III system and are associated with increased mortality (12). However, APACHE III score and other disease severity score, such as simplified acute physiology score (SAPS) II have not specifically evaluated for the purpose of discrimination between infectious and non-infectious fever in the ICU.
In the present study, we evaluated the value of serum PCT, HMGB1, SAPS II, and APACHE III scores in the differentiation between infectious and non-infectious fever in ICU patients.
MATERIALS AND METHODS
Study population
A prospective cohort study was conducted at the 21-bed medical intensive care unit (MICU) of Chung-Ang University Hospital, Seoul, Korea, from August 2008 to February 2009. This study was approved by the IRB of Chung-Ang University Hospital and the approval number was C2008015(118). Informed consent was obtained from the family members of the patients.
During the 7-month period (August 2008 to February 2009), 448 patients were consecutively admitted to the MICU. Fever developed in 63 of these patients (14.1%). Thirty-five patients were men and 28 were women, and the mean age was 65.2±12.4 yr. Fever developed within three days of admission in 46 of the 63 patients. The mean duration of ICU stay was 25.8±20.2 days, and the mean duration of fever was 3.0±2.4 days. The SAPS II and APACHE III scores were 11.2±3.8 and 45.3±19.5, respectively (Table 1).
Measurement of clinical and laboratory parameters
Body temperature was measured using the axillary method with an electronic thermometer (Thermoval classic, PAUL HARTMANN AG, German). We defined ICU fever as a body temperature above 38.3℃ that developed 48 hr after ICU admission. Within 24 hr after the development of fever, serum samples were collected and stored at -70℃ and serum PCT and HMGB1 levels were measured later with duplication. A fluorescent enzyme immunoassay (FEIA) (VIDAS BRAHMS PCT, France) was used to measure PCT levels. Serum HMGB1 levels were evaluated with an enzyme-linked immunosorbent assay (HMGB1 ELISA kit, Shino-Test Co, Japan). Clinical parameters, including demographic data, underlying diseases, duration of ICU stay, causes of fever, SAPS II, APACHE III scores, and mortality rate were also analyzed.
Diagnostic criteria for the cause of fever
Pneumonia was defined as a constellation of symptoms and signs in combination with at least a newly developed infiltrate upon chest radiography. Urinary tract infection (UTI) was defined as pathogenic microorganisms detected in the urine at more than 100,000 organisms/mL (13). Sepsis was defined as systemic inflammatory response syndrome (SIRS) with a proven or suspected microbial etiology (14). Phlebitis was defined as the clinical findings of pain, tenderness, induration, and/or erythema in a superficial vein due to inflammation, infection, and/or thrombosis (15). Post-operative fever was defined as non-infectious fever occurring within the first 4 post-operative days, based on a modification of the description by Clarke et al. (16). Drug fever was defined as a disorder characterized by fever coinciding with the administration of a drug and disappearing after the discontinuation of the drug, when no other cause for the fever was evident after a careful physical examination and laboratory investigation. Fevers were labeled as unknown cause when routine medical and laboratory examination did not reveal the origin of fever.
Causes of fever
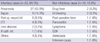
Most fevers were due to infectious causes (53 cases, 84.1%). Pneumonia (27 cases, 42.9%) was the most common cause of infectious fever. Other causes of infectious fever were sepsis, postoperative wound infection, and urinary tract infection. Causes of non-infectious fever (10 cases, 15.9%) included drug fever, gastrointestinal bleeding, and postoperative fever (Table 2).
Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences version 17.0 (SPSS, Inc., Chicago, IL, USA). Continuous variables were compared using the Student t test for normally distributed variables and the Mann-Whitney U test was used for non-normally distributed variables. P values of less than 0.05 were considered significant. The ability of each parameter to discriminate between infectious and non-infectious fever was investigated using a receiver operating characteristic (ROC) analysis.
RESULTS
There were no significant differences in age (P=0.19), gender (P=0.76), serum HMGB1 (P=0.52), and mortality rate (P=0.33) between patients with infectious and non-infectious fever (Table 1). Febrile patients with infectious causes had higher levels of serum PCT than those with non-infectious causes (7.8±10.2 vs 0.5±0.2 ng/mL, P=0.026). In addition, infectious fever was associated with higher SAPS II and APACHE III scores (12±3.8 vs 7.6±2.7, P=0.006; 48±20 vs 28.7±13.3, P=0.039) (Table 1).
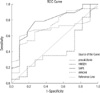
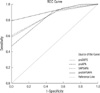
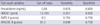
The Receiver Operating Characteristic (ROC) curve analysis revealed that the diagnostic performance of PCT and the SAPS II and APACHE III scores for infectious and non-infectious fever was in the good range, and the area under the curve (AUC) was 0.726 (95% CI; 0.587-0.865) for PCT, 0.759 (95% CI; 0.597-0.922) for the SAPS II score, and 0.715 (95% CI; 0.550-0.880) for the APACHE III score (Fig. 1). The optimum cutoff value for distinguishing between infectious and non-infectious fever was 0.68 ng/mL for PCT (sensitivity, 67.6%; specificity, 80.0%), 8.5 points for the SAPS II score (sensitivity, 78.4%; specificity, 70.0%), and 31.5 points for the APACHE III score (sensitivity, 64.9%; specificity, 70.0%) (Table 3), respectively. The combination of PCT, SAPS II and APACHE III scores increased the AUC and diagnostic accuracy (Fig. 2). When we set the cut off value of PCT to 0.68 ng/mL, SAPS II to 8.5 points, and APACHE III to 31.5 points, the combination of all three parameters showed 100% of sensitivity, 25% of specificity, 43% of positive predictive value, and 100% of negative predictive value for the differentiation between infectious and non-infectious fever.
DISCUSSION
In the present study, we evaluated biologic markers, including serum PCT and HMGB1, and disease severity scores, such as SAPS II and APACHE III, in the differentiation of infectious and non-infectious fever in the ICU. In accordance with the guidelines of the Society of Critical Care Medicine and the Infectious Disease Society of America, we defined an ICU fever as a temperature equal to or above 38.3℃ in patients who stayed in the ICU for at least 48 hr (3).
In the present study, fever developed in 63 patients among 448 consecutive patients admitted to the ICU (14.1%), which was far less as compared to other report (2). The low prevalence of ICU fever in our study might be explained by the fact that we evaluated patients admitted to the medical ICU and excluded patients in the surgical ICU, where fever can be due to many causes, such as wound infection, transfusion reaction, and postoperative fever. Also, our ICU contains a coronary care unit (CCU), and these patients usually have a low risk for infectious disease. In addition, we used the axillary method to check body temperature, and this method usually results in lower temperature compared to other methods (17, 18).
ICU patients frequently have multiple infectious and noninfectious causes of fever, necessitating a systematic and comprehensive diagnostic approach. The most common infection reported in ICU patients is pneumonia, followed by sinusitis, blood stream infection, and catheter-related infection (2, 4, 19). As was reported in our previous study, infectious causes of fever (84.1%) predominated, and pneumonia was the most common cause of infection (42.9%) in the present study (20). While infections are important causes of fever in the ICU, many noninfectious inflammatory conditions result in tissue injury, inflammation, and a febrile reaction. Noninfectious disorders that should be considered in ICU patients are post-operative fever, transfusion reaction, drug fever, and cerebral infarction (15). In the present study, causes of non-infectious fever (10 cases, 15.9%) were drug fever, gastrointestinal bleeding, and postoperative fever (Table 2).
It is well known that early recognition, together with prompt and appropriate treatment of infections, can significantly reduce mortality in critically ill patients (2). The dilemma with ICU fever is to exclude noninfectious causes as soon as possible and then to locate the site of infection and determine the likely pathogens. To date, no single clinical or biological indicator has gained unanimous acceptance in the differentiation between infectious and noninfectious fever in the ICU.
CRP and PCT have been used as objective markers of bacterial infection. Although CRP is a more sensitive marker of sepsis than either body temperature or white blood cell count, it lacks specificity (21). PCT, a propeptide of calcitonin, is found to be an earlier marker of septic shock than CRP and it correlates more closely to severity of disease (22). Pleural effusion PCT was higher in bacterial pneumonia than in non-bacterial infection (23). However, there is a debate for the utility of PCT in distinguishing infection from other causes of systemic inflammatory response syndrome (SIRS) in older patients (24). In the present study, we were able to confirm that serum PCT levels were significantly high in patients with infectious fever (Table 1). Manufacturer's instruction recommends interpreting PCT results with the five categories indicating healthy condition, local infection, sepsis, severe sepsis, and septic shock. However, in the present study, the mean value of PCT in 9 patients with sepsis (6.9 ng/mL) was not different from that of other patients with local infection (7.8 ng/mL).
We also evaluated serum HMGB1 for this purpose because there is abundant evidence supporting the role of HMGB1 as an inflammatory mediator, especially in sepsis (9, 10). To our disappointment, serum HMGB1 proved not to be useful as a tool in the differentiation between infectious and non-infectious fever (Table 1). In the present study, disease severity scores, including the SAPS II and APACHE III scores, were different between infectious and noninfectious fever (Table 3) (Fig. 1). The overlap between the two groups was too large to be used in the differentiation of infectious and non-infectious fever. However, combination of each parameter and especially combination of all three parameters, PCT, SAPS II, and APACHE III score increased AUC and diagnostic accuracy for the differentiation (Fig. 2). Because there is no single clinical or biological indicator that gained unequivocal acceptance in the differentiation between infectious and noninfectious fever in the ICU, the combined analysis of all three parameters might be a practical alternative for this purpose.
Our study has a few limitations. First, we performed the study at only one hospital and evaluated only patients admitted to the medical ICU. We were able to identify candidate parameters for the differentiation of infectious and noninfectious fever (serum PCT, SAPS II, and APACHE III scores). However, there is a limitation in the diagnostic accuracy of three parameters. Despite these limitations, our study may be the rare, prospective study in Korean population to evaluate parameters for the differentiation between infectious and noninfectious fever in the ICU.
In conclusion, serum PCT levels, SAPS II and APACHE III scores demonstrated significant differences between patients with infectious and non-infectious fever and combined analysis of all three parameters increased diagnostic accuracy.

 XML Download
XML Download