

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spontaneous regression of a malignant tumor is very rare. It has been estimated that this occurs less than once in 60,000 to 100,000 people with cancer and about 20 such cases have been reported annually (1, 2). Spontaneous regression of a malignant tumor has often noted in hypernephroma, neuroblastoma, malignant melanoma, choriocarcinoma, bladder cancer, but this is extremely rare for stomach cancer (3). We recently experienced a case of spontaneous regression of advanced gastric cancer, Borrmann type IV, and we report on our case along with a review of the related literature.
CASE REPORT
An 84 yr-old male with a history of nausea and vomiting for the previous 3 weeks was admitted to our hospital. He used no medicine or herbal material except for an oral hypoglycemic agent for diabetes mellitus for 10 yr. His vital signs were stable and the physical examination revealed a palpable mass at the epigastrium. On laboratory examination, the WBC was 7,630/µL, the hemoglobin level was 14.2 g/dL, platelet 194,000/µL, fasting glucose 140 mg/dL, blood urea nitrogen 24.6 mg/dL, creatinine 1.25 mg/dL, total protein 6.62 g/dL, albumin 3.49 g/dL, AST 18 IU/L, ALT 13 IU/L, total bilirubin 0.41 mg/dL, direct bilirubin 0.18 mg/dL, alkaline phosphatase 126 IU/L, γ-GTP 11 IU/L, the prothrombin time (INR) was 1.0 and the activated partial thromboplastin time was 23.0 sec.
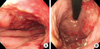
Esophagogastroduodenoscopy (EGD) showed rugal fold thickening and widening along the whole length of the gastric body. The mucosa was congested and it looked dysplastic. When touched with biopsy forceps, the mucosa showed friability and bleeding to easy touch (Fig. 1). Since the time of discharge, he took famotidine and itopride HCL without any other medication or herbal medication and he revisited our hospital for follow up 6 months later. EGD showed that the gastric folds were well distended by air inflation and the mucosa looked normal at the previously dysplastic and friable areas from the cardia to the lower body (Fig. 2).
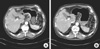
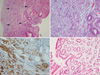
Abdominal computerized tomography (CT) revealed diffuse irregular wall thickening and mucosal enhancement from the cardia to the lower body. Perigastric infiltration was present, yet lymph node enlargement or distant metastatic lesion was not identified (Fig. 3A). Multiple pieces of mucosal biopsy were obtained and the histological examination showed poorly differentiated adenocarcinoma (Fig. 4A-C). Malignant cells were stained at Periodic acid Schiff (PAS) stain and immunohistochemical stain was positive for cytokeratin AE1/AE3 and negative for LCA. Finally, we diagnosed the patient as suffering with advanced gastric cancer, Borrmann type IV, stage II (T3N0M0) and we planned surgical resection. But patient refused surgical resection and chemotherapy on consolation and then he was discharged. Abdominal CT revealed decreased wall thickening of the body compare to that of 6 months ago. The perigastric infiltration had regressed (Fig. 3B). The histology showed no evidence of malignancy (Fig. 4D). We examed DNA test (DNA fingerprinting) using autosomal short tandem repeat to know whether the two biopsy specimens were from the same patient. And the result of DNA test revealed that the DNA of two specimens were identical. The patient is alive without any digestive symptoms 14 months after the follow up exam.
DISCUSSION
According to Everson's definition, spontaneous regression of malignant tumor is partial or complete disappearance of a malignant tumor in the absence of treatment that is ordinarily considered to be capable of producing regression. Further, the regression need not progress to complete disappearance of the tumor (4). This is very rare phenomenon. Of the 741 cases of spontaneous regression of malignant tumor from the year 1900 year to 1987, nine types of tumor (hypernephroma, malignant melanoma, neuroblastoma, retinoblastoma, leukemia, lymphoma, breast cancer, bladder cancer and choriocarcinoma) were noted in 511 cases (69%) and stomach cancer was noted in 17 cases (2.29%) (3). Regarding gastric cancer, 19 cases (5) of spontaneous regression have been reported.
Spontaneous regression of malignant tumor is very rare and its cause is mostly ambiguous, so it is very difficult to determine the scientific mechanism. Yet the mechanisms suggested till now are a hormonal or immunological mechanism, operative trauma, necrosis or vascular insufficiency, infection and a psychological mechanism (1, 3).
A hormonal mechanism was suggested because the onset of a pregnancy (6) or the cessation of ingestion of oral contraceptives was associated with the onset of a spontaneous regression of tumor (7, 8). In many cases of renal cell carcinoma, the remaining tumor mass regressed after the primary tumor or metastases had been surgically resected (9, 10), so we can presume that host immune system can destroy remaining tumor after the removal of the tumor burden (11). Other important mechanism is a febrile response associated with infection (12, 13). Of the patients with lung cancer, the 5-yr survival is increased in patients who are complicated with postoperative empyema (14). It was also reported that a patient with hepatocellular carcinoma developed severe cholangitis due to choledocholithiasis, and then hepatectomy was performed but the resected tumor demonstrated complete necrosis (15). In addition, some authors suggested a psychological factor (16) as the possible mechanism, but the evidence on this is still not clear.
At first, we suspected that the biopsy specimens could be mistaken. But, it was proven that the DNA of two specimens were identical according to the results of DNA fingerprinting. And the patient had no twin brother. So we could conclude that it was the spontaneous regression of advanced gastric cancer.
In this case, we could not identify any possible reason for the spontaneous regression of advanced gastric cancer. We herein report this very rare case, with a review of the related literature, in which advanced gastric cancer spontaneously regressed in 6 months without any clear cause.

 XML Download
XML Download