

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Impaired lung function, as measured by forced vital capacity (FVC) or forced expiratory volume in one second (FEV1), is known to be associated with increased prevalence and mortality of cardiovascular diseases (1-3). Among the various cardiovascular risk factors, previous studies suggest the association of impaired lung function with insulin resistance (IR) and type 2 diabetes mellitus (4, 5). Furthermore, decreased FVC or FEV1 has been shown to be associated with persistent low grade systemic inflammation assessed by increased serum inflammatory markers, such as C-reactive protein (CRP) (5).
Metabolic syndrome (MetS) refers to a cluster of abdominal obesity, dyslipidemia, hypertension, insulin resistance (IR), and prothrombotic states that predisposes to cardiovascular disease (6). Recently, many epidemiologic studies have highlighted the role of systemic inflammation in atherosclerosis and cardiovascular disease (6, 7). Moreover, considerable attention is being paid to the relationship between systemic inflammation, IR and MetS (8, 9).
Although recent studies suggest the association of impaired lung function with MetS (10-13), such studies have several limitations such as, small number of elderly study population (11), inclusion of smokers (10-12), and insufficient consideration for IR or systemic inflammatory markers (10-13). There have been few studies investigating the relationship between lung function and systemic inflammation, IR, and MetS simultaneously in a large number of nonsmoking healthy subjects. We therefore incorporated all components of MetS, IR, high-sensitivity (hs) CRP as a systemic inflammatory marker, and lung function variables into the analysis, and assessed the relationships in 9,581 adult nonsmoking Korean males. We also evaluated whether the risk increases in a severity-dependent manner even within normal range of lung function.
MATERIALS AND METHODS
Subjects
Between January to September 2005, a total of 33,546 male subjects, who were inhabitants of either Seoul or Gyeonggi-do, Korea underwent a health examination at the Health Promotion Centre in Kangbuk Samsung Hospital (a 640-bed tertiary university hospital in Seoul, Korea). Among them, we recruited nonsmoking male subjects, in whom data for pulmonary function test, hs-CRP level and MetS parameters were available. Those subjects with a history of malignancy, asthma, chronic lung disease, pulmonary tuberculosis, liver disease, and severe cardiovascular disease were excluded. Final analysis was performed on 9,581 subjects. Self-reported alcohol intake, and physical activity habits were obtained from questionnaire response. Ethics approval for patient recruitment and analysis of the data were obtained from the institutional review board of Kangbuk Samsung Hospital (KBC 09093).
Measurement of lung function
Spirometry was performed as recommended by the American Thoracic Society (14), using Vmax 22 (SensorMedics, Yorba Linda, CA). Absolute values of FVC and FEV1 were obtained and the percentage of predicted values (% pred) for FEV1 and FVC were calculated from following equations obtained in a representative Korean population (15).
Predicted FVC=-4.8434-(0.00008633×age2 [years])+(0.05292×height [cm])+(0.01095×weight [kg])
Predicted FEV1=-3.4132-(0.0002484×age2 [years])+(0.04578×height [cm])
The highest FVC and FEV1 value of the three or more tests with acceptable curves was used. Ventilatory patterns were defined as normal (FVC ≥80% and FEV1/FVC ≥0.7), restrictive (FVC <80% and FEV1/FVC ≥0.7; n=1,197; 12.5%), or obstructive pattern (FEV1/FVC <0.7; n=134; 1.4%). In addition to ventilatory patterns, we also classified the patients according to the quartiles of FVC or FEV1 (% pred). Based on the FVC (% pred), the resulting four categories were as follows: quartile 1, <85%; quartile 2, ≥85%, <93%; quartile 3, ≥93%, <101%; quartile 4, ≥101%. In the same way, based on the FEV1 (% pred), the subjects were also divided into quartiles: quartile 1, <85%; quartile 2, ≥85%, <92%; quartile 3, ≥92%, <100%; quartile 4, ≥100%.
Anthropometric measurements and blood test
Systolic (SBP) and diastolic blood pressure (DBP) were measured according to the hypertension Detection and Follow-up Program protocol by using a mercury blood pressure device after the subjects had rested longer than 5 min (16). For the cases with a SBP higher than 140 mmHg and a DBP higher than 90 mmHg, the BP was measured two more times after resting, and the average value was used. Body mass index (BMI) was calculated by weight (kg) divided by the squared height (m) (kg/m2). The waist circumference (WC) was measured in the standing position, at the level of umbilicus, located midway between the lower costal margin (bottom of lower rib) and the iliac crest (top of pelvic bone). After 12 hr of fasting, blood glucose (FBG), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein-cholesterol (LDL-C) levels were obtained. The hexokinase method (Advia 1650 Autoanalyzer; Bayer Diagnostics, Leverkusen, Germany) was used to measure blood glucose levels and an enzymatic colorimetric test was used to measure TC and TG levels. The selective inhibition method was used to measure HDL-C and a homogeneous enzymatic colorimetric test was used to measure LDL-C. The fasting serum insulin level was measured by immunoradiometric assay (RIABEAD II, Abbott, Tokyo, Japan), having an intra-assay coefficient of variance of 1.2% to 1.9% and an inter-assay coefficient of variance of 1.4% to 3.3%. Serum hs-CRP levels were measured using a nephelometric assay (BNII nephelometer, Dade Behring, Deerfield, IL, USA). The results were presented as milligrams per liter, and the limit of measurement was 0.175 mg/L with a sample dilution of 1:20.
Insulin resistance status was calculated by using the homeostatic model assessment-insulin resistance (HOMA-IR) (17). The calculation formula was as follows:
HOMA-IR=(fasting insulin [µIU/mL]×fasting blood glucose [mM/L])/22.5
Definition of presence of metabolic syndrome
Based on the American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI) criteria with the WC defined by the Western Pacific Region of WHO for obesity (WPRO) criteria, the diagnosis of MetS was made when the subject satisfied more than 3 categories among the 5 categories described below (6, 18): 1) Abdominal obesity: WC ≥90 cm; 2) TG ≥150 mg/dL; 3) HDL-C <40 mg/dL; 4) Hypertension ≥130/85 mmHg; 5) FBG ≥100 mg/dL.
Statistical analysis
Statistical analysis was performed with PASW statistics v.17.0 package for Windows (SPSS Inc., Chicago, IL, USA). Data are presented as mean±SD. Descriptive statistics were used to describe the study population at baseline. The assessment for the normality of the variables was done with Kormogorov-Smirnov test, and the hs-CRP values were log-transformed as they did not follow normal distribution. The comparisons of mean values of the variables among the subdivided groups were performed by Kruskal-Wallis test or one-way ANOVA, and multiple comparison tests were performed with post hoc analysis. The chi-square test was used for cross-tabulation analysis. Stepwise multiple logistic regression analyses were performed to evaluate the associations between hs-CRP, HOMA-IR, MetS and the presence of lowest FVC and FEV1 (% pred) quartile after adjustment for confounding factors, such as age and BMI. A 95% confidence interval (CI) was determined for each risk. For all statistical tests used, P value <0.05 was considered significant.
RESULTS
Ventilatory patterns and metabolic syndrome, HOMA-IR, and hs-CRP
Clinical characteristics of the study population based on the ventilatory patterns are presented in Table 1. The mean age of the 9,581 participants was 40.9±8.9 yr. The prevalence of MetS was 19.3% for the whole subjects. Individuals in the restrictive pattern were more likely to have higher prevalence of MetS, to have higher WC, SBP, DBP, HOMA-IR, to have higher concentration of FBG, TG, TC, LDL-C, and to have lower levels of HDL-C. The crude odds ratio (OR) of MetS for restrictive pattern was 1.71 (95% CI, 1.49-1.96). After adjustment of age, BMI, and physical activity, MetS and hs-CRP remained significant risk factors for restrictive pattern (adjusted odds ratio [ORa] [95% CI], 1.55 [1.12-2.14] for MetS and ORa, 1.32 [1.16-1.50] for hs-CRP). Those patients with obstructive pattern showed significantly higher hs-CRP concentration compared with other groups. Multiple logistic regression analysis revealed that only hs-CRP was independently associated with obstructive pattern (1.28 [1.02-1.61]). However, the OR and ORa of MetS for obstructive pattern were 1.11 (0.73-1.70) and 1.39 (0.66-2.94), respectively.
Quartiles of FVC and FEV1 (% pred) and component of metabolic syndrome
The mean values of BMI, WC, BP, serum FBG, TC, TG, LDL-C and insulin levels increased as the quartiles of FVC and FEV1 (% pred) decreased from quartile 4 to quartile 1. Mean HDL-C value decreased from quartile 4 to quartile 1 (Table 2).
Quartiles of FVC and FEV1 (% pred) and HOMA-IR, hs-CRP
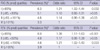
Mean HOMA-IR significantly increased as the FVC or FEV1 (% pred) decreased from quartile 4 to quartile 1. On post hoc analysis, the differences were significant among all groups (P<0.01). Those patients with lowest FEV1 (% pred) (Quartile 1) had a significantly higher hs-CRP concentration compared with other three groups (Quartile 2, 3, 4) (Table 3).
Prevalence and odds ratio for the risk of MetS according to quartiles of FVC and FEV1 (% pred)
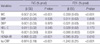
The lower quartile of FEV1 and FVC were independently associated with MetS. After adjustment for age and BMI, MetS significantly associated with reduced lung function (ORa [95% CI], 1.21 [1.02-1.44] for FVC (% pred) quartile 1 and ORa, 1.38 [1.17-1.63] for FEV1 (% pred) quartile1 when the highest quartile was considered as the reference category (Table 4).
Multiple logistic regression analyses with lowest quartile of FVC and FEV1 (% pred) as the dependent variables
Stepwise multiple logistic regression analyses were performed to determine the relationship between the presence of the lowest FVC and FEV1 (% pred) quartile and hs-CRP, HOMA-IR, and MetS after adjustment of age and BMI (Table 5). These analyses showed that higher hs-CRP, HOMA-IR, and abdominal obesity were independent predictors of the lowest FVC and FEV1 (% pred) quartiles. Similar results were obtained when the multiple linear regression analyses were repeated using FVC and FEV1 (% pred) as a continuous variables without dividing into quartiles (Table 6).
DISCUSSION
The major finding of this study is that when the study population was divided into quartiles based on FVC or FEV1 (% pred), there were significant increase in the prevalence of MetS, risk of being insulin resistant, and concentration of serum hs-CRP as the lung function decreased even within normal range of lung function. Multiple logistic regression analysis revealed that abdominal obesity, HOMA-IR, and serum hs-CRP are independent risk factors for the lowest lung function. Moreover, according to the results based on ventilatory patterns, MetS was more significantly related with restrictive pattern, and hs-CRP was a significant risk factor for both restrictive and obstructive pattern. These results clearly indicate that lung function and serum hs-CRP, IR and MetS are closely related.
One of the strong points we observed in this study was that systemic inflammation as determined by hs-CRP was strongly related to both the restrictive and obstructive ventilatory pattern as well as inversely linked with lowest FVC or FEV1 (% pred) quartile, suggesting a crucial role in the decline of lung function. These results extend previous finding demonstrating an association of increased CRP level with lung function decline (19), or obstructive and restrictive lung diseases (20). Aronson et al. (21), also showed inverse association between lung function and CRP level in apparently healthy subjects and in the subgroup of never-smokers. Considering the facts that adipokines secreted by visceral adipose tissue can negatively affect lung function (22) and that WC is known to be the main determinant of elevated CRP in MetS (23), a plausible mechanism for the inverse association between systemic inflammation and reduced lung function in this study could be best explained by the role of MetS or abdominal obesity. Adipokines promote systemic inflammation, which subsequently may lead to activate airway inflammation and decline in lung function. However, it is still unclear whether initially higher level of systemic inflammation may accelerate lung function decline. In 16 years of follow-up study in elderly by Jiang et al. (24), baseline CRP levels failed to show significant correlation with future lung function, whereas baseline fibrinogen levels showed inverse correlation with future lung function. To fully elucidate this association, a large prospective study would be needed.
This study showed that the risk of being relatively insulin resistant, as measured by HOMA-IR, was significantly increased as the lung function decreased. We also found that together with hs-CRP, HOMA-IR was the independent risk factor for reduced FVC, FEV1 (% pred). Our study clearly demonstrated a direct impact of the MetS or IR per se on the development of reduced lung function in a severity-dependent manner even after adjustment for confounding factors. There have been a few studies that analyzed the relationship between lung function and HOMA-IR. In the longitudinal 7-yr follow-up study performed in initially nondiabetic 1,436 males and 896 females by Engström et al. (25), subjects with a reduced FVC had an increased risk of developing IR, defined by highest quartile of HOMA-IR. In another study by Lawlor et al. (5), HOMA score decreased as FEV1 and FVC increased in 3,911 women enrolled in British Women's Heart and Health Study. As both reduced lung function and the presence of IR have been associated with increased cardiovascular mortality, the coexistence or the association of IR with reduced lung function might have considerable impact on future health.
Previous studies have reported that reduced lung function is associated with MetS (10-13). In a recent study performed in 2,396 Japanese, Nakajima et al. (12), showed that CRP levels and FVC (% pred), but not FEV1/FVC, were significantly associated with MetS. They also demonstrated that restrictive lung function was associated with MetS in a severity-dependent manner. Nonetheless, their study had an important limitation like the study by Lin et al. (10), in that IR status was not considered in the evaluation, which is the most fundamental element for the association between reduced lung function and MetS. Leone et al. (13) also reported a positive independent relationship between lung function impairment (both obstructive and restrictive pattern) and MetS in a recent large population-based study, in which abdominal obesity was found to be playing a core role. However, IR and systemic inflammation were not assessed adequately in their analysis. Moreover, another important limitation in the majority of previous studies was that they only focused on the relationship between the abnormal lung function and MetS. Engström et al. (25) identified that the risk for the future development of IR has decreased by ten percent for each ten percent increase in FVC1 (% pred). In the National Health and Nutritional Examination Survey follow-up study, Sin et al. (26) also found that even a modest decline in FEV1 (% pred) from a mean of 109% to 88 % was associated with a five-fold increase in mortality from ischemic heart disease. Based on these results, we assumed that it is more reasonable to analyze the relationship between lung function, systemic inflammation, IR and MetS, further expanding to the categories above the normal range of lung function whether there is a stepwise increment in the relative risk for the development of IR and MetS as the lung function decreases. In this study, the prevalence and the risk for MetS gradually increased as the both FVC and FEV1 (% pred) decreased from highest to lowest quartile. This observation is consistent with our assumption that the prevalence of MetS increases even within the normal range of FVC and FEV1 (% pred). However, it is difficult to draw clear conclusion about cause-effect relationship or clinical impact based on this study alone. Further studies are required to clarify the causal relationship and to assess clinical outcomes including long-term changes in lung function as well as the therapeutic effect of MetS on the rate of lung function decline.
There are several explanations for the relationship between reduced lung function and MetS. MetS is a cluster of disease comprised of multiple cardiovascular risk factors such as IR, dyslipidemia, glucose intolerance and hypertension, most of which could stem from one cause, visceral obesity (27). Obesity has long been shown to be related to cause physiologic impairments in respiratory system (28): airflow limitation with reduction of both FEV1 and FVC; reduction in lung volumes, especially expiratory reserve volume (ERV) and functional residual capacity (FRC), which predispose toward a decrease in peripheral airway diameter; reduction in respiratory system compliance, as well as an increase in oxygen cost of breathing and airway hyperresponsiveness (AHR). Taken together, decrease in retractive forces of the lung parenchyma on the airways at low lung volume in obese people, lead to reduce airway caliber and increased AHR, which potentially causing detrimental effect on lung function. The association of obstructive lung function with MetS could be explained by obesity, and subsequent systemic inflammation and by the role of adipokines (29).
This study has several limitations. First, because obstructive pattern was found only in 1.4% of these participants without post-bronchodilator assessment and the diagnosis of restrictive pattern was made without total lung capacity measurement, analysis according to the ventilatory patterns was not sufficiently adequate. Moreover, since FEV1 is dependent on the FVC, quartiles of FEV1 values may not exclusively reflect the degree of true airflow limitation. Further clinical studies are warranted exploiting the measurement of total lung capacity and bronchodilator test to precisely define the ventilatory patterns. Second, since this study used a cross-sectional design, longitudinal studies are needed to investigate the interactions between lung function, inflammation, IR, MetS and their relation with future cardiovascular disease. In addition, though we found statistically significant trend, the differences between values of metabolic parameters in lung function quartiles were small. The clinical significance of these small differences remains to be elucidated, and needed to be verified in future prospective longitudinal study, whether small different degree of metabolic perturbations would be associated with different incidence of cardiovascular events or different rate of lung function decline.
In conclusion, this study clearly showed that metabolic syndrome, insulin resistance, and systemic inflammation are important risk factors for reduced lung function in nonsmoking Korean males.




 XML Download
XML Download