

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Resistance to thyroid hormone (RTH) is a rare an autosomal dominant hereditary disorder (1). In the majority of cases, RTH is caused by mutations in the thyroid hormone receptor beta (TRβ) gene. The clinical presentation is variable, but common features include goiter, an absence of the classic thyrotoxic symptoms and metabolic consequences of elevated thyroid hormone levels, and a normal or exaggerated thyroid stimulating hormone (TSH) response to thyrotropin-releasing hormone (TRH). Until now over 1,000 cases have been identified around the world, and nine cases have been reported in Korea (2-9).
We recently encountered a case of RTH with incidental micropapillary thyroid carcinoma. The association between RTH and thyroid cancer has not yet been clarified, but there is evidence to suggest that RTH may play a contributory role.
Here, we present a case of RTH with thyroid cancer along with the mutation analysis for the TRβ gene.
CASE REPORT
A 38-yr-old Korean woman visited a private clinic for the evaluation of anterior neck swelling. The initial laboratory examination revealed an elevated levels of serum thyroid hormone without accompanying TSH suppression (free T4 2.67 ng/dL [range, 0.64-1.72] and TSH 1.82 µIU/mL [range, 0.4-4.5]). She had no signs or symptoms of typical thyrotoxicosis except diffuse goiter and mild palpitations. However, due to findings of elevated serum thyroid hormone levels and goiter, she was diagnosed with Graves' disease, and prophylthiouracil (PTU) was prescribed. After three months of PTU (100 mg three times daily), she complained of generalized weakness, a weight gain of about 3 kg, and generalized edema. Consequently, she was referred to our hospital.
When first seen at our hospital on December 9, 2008, her height and weight were 162 cm and 49 kg, respectively, with a blood pressure of 97/68 mmHg and a pulse rate of 96 beats/min. Her thyroid gland was symmetrically enlarged, and exophthalmos and myxedematous skin lesions were absent. Past medical history was significant for goiter first detected at age 13. At that time, the physician recommended regular checks for thyroid function because of elevated levels of thyroid hormones, but she was lost to follow-up. Her family history included one sister who had a diffuse goiter and a thyroid nodule.
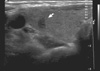
The laboratory examination revealed an elevated level of TSH despite an elevated levels of thyroid hormone [total T3 181 ng/dL (range, 76-190), free T4 2.50 ng/dL and TSH 10.23 µIU/mL]. Thyroid autoantibodies against thyroperoxidase, thyroglobulin, and TSH-receptor were all negative. Thyroid ultrasonography (USG) revealed several micro-nodules in both lobes. USG-guided fine-needle aspiration was performed for the nodule which showed suspicious features of malignancy in the right thyroid lobe (Fig. 1), and the cytologic diagnosis was papillary thyroid carcinoma. A 99m technetium thyroid scan showed diffuse enlargement of the thyroid gland with increased uptake (10.1%) (Fig. 2). PTU was discontinued due to TSH elevation and the occurrence of hypothyroid symptoms. After PTU was stopped for one month, hypothyroid symptoms disappeared and thyroid function tests (TFTs) revealed elevated thyroid hormone levels [free T4 2.20 ng/dL and total T3 141 ng/dL] and a nearly normal level of TSH (5.60 µIU/mL).
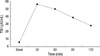
The differential diagnosis at this point was between RTH and a TSH-secreting pituitary adenoma based on the TFTs findings. TSH-secreting pituitary adenoma was ruled out because the patient had no clinical features of thyrotoxicosis, a negative MRI of the pituitary gland, a normal level of the α-subunit of TSH (0.36 mIU/mL, range, 0-0.9), and an exaggerated response of TSH to a thyrotropin-releasing hormone (TRH) stimulation test (Fig. 3).
Accordingly, genomic DNA was isolated from the peripheral blood leukocytes of the patient with a G-DEX™ Ilb Genomic DNA Extraction Kit (Intron Biotechnology, Seongnam, Korea). PCR amplification was conducted on seven coding exons (from exon 4 to 10) of the TRβ gene. The sequences were analyzed using the computational software ABI 3730 XL (Applied Biosystems, Foster City, USA). A point mutation was detected in exon 9 of the TRβ gene that caused the substitution of threonine (ACG) for methionine (ATG) at codon 310 (M310T). This mutation has not yet been reported in Korea. The patient's sister had normal TFTs and no mutation by DNA sequencing analysis (Fig. 4).
Ultimately, the patient was diagnosed with RTH and papillary thyroid carcinoma. She underwent a total thyroidectomy and the pathologic diagnosis was two micropapillary thyroid carcinomas in both lobes (0.4 cm in the right and 0.2 cm in the left lobe). After surgery, she received levothyroxine (L-T4) at 150 µg/day). After three months of L-T4 therapy, her TSH level was still elevated (TSH 45.1 µIU/mL) and she complained about symptoms of hypothyroidism; therefore, we increased the dose of L-T4 to 200 µg/day. After two months, her TSH level decreased to 15.5 µIU/mL, and most of her hypothyroid symptoms disappeared. Ultimately the dose of L-T4 was increased to 250 µg/day titrated to achived a TSH level comparable to the preoperative value.
DISCUSSION
Inappropriate secretion of TSH and the co-existence of elevated thyroid hormone has been noted in several circumstances, including intermittent administration with L-T4, TSH-secreting pituitary adenoma, and RTH (10). RTH is distinguished from TSH-secreting pituitary adenoma by an exaggerated response to TRH, normal levels of the TSH α subunit, and a normal pituitary gland on sella-MRI. RTH is characterized by reduced clinical and biochemical manifestations of thyroid hormone action relative to the elevated circulating thyroid hormone levels. The linkage between RTH and the TRβ gene was detected in 1988 (11). About 90% of RTH patients carry mutations in the T3-binding domain between exon 4 and exon 10 of the TRβ gene. The majority of previously described mutations were missense mutations that induced single amino acid substitutions.
Most patients of RTH are clinically euthyroid, some individuals may appear to be hypothyroid or hyperthyroid. Furthermore, the same subject can manifest signs and symptoms of hypothyroidism in one tissue, while the findings may be suggestive of thyrotoxicosis in other tissues (1). On the basis of clinical features, three different forms of RTH have been described: generalized RTH (GRTH), pituitary RTH (PRTH), and peripheral tissue RTH (PTRTH). GRTH patients, the most common form, appear eumetabolic despite elevated level of thyroid hormones maintained by the hypersecretion of TSH in response to hypothalamic TRH. PRTH patients generally display thyrotoxic. Administration of an anti-thyroid drugs may improve the symptoms. PTRTH patients manifest symptoms and signs of hypothyroidism, despite of normal serum thyroid hormone and TSH levels (12).
Treatment of RTH should be aimed at maintaining a normal metabolic status. In our case, administration of anti-thyroid drugs under the misdiagnosis of Graves' disease resulted in an increase in serum TSH and the appearance of symptoms of hypothyroidism, while thyroid hormone levels remained elevated. As expected, large amounts of L-T4 were needed in our patient after total thyroidectomy. Titration should be achieved by assessing tissue responses. Restoration of the preoperative levels of TSH is the recommended target in GRTH.
The RTH in our patient was accompanied by two small papillary thyroid cancers. The precise contribution of RTH to thyroid tumorigenesis is not fully understood, but there is evidence to suggest that they may play contributory roles. About 95% of RTH patients have diffuse goiter, and continuous stimulation of the thyroid by excess TSH may be related to the formation of thyroid nodules and the growth of thyroid cancer (13). Previous pathological examinations of the thyroid in RTH cases have revealed hyperplasia of the follicular epithelium, sometimes accompanied by papillary proliferation probably due to continuous stimulation by TSH (12). Not only the effect of thyroid, but the cases of co-existence of pituitary tumor were reported (14). TRβ mutants may also have oncogenic actions. Abnormal expression and somatic mutation at various sites of the TRβ gene have been described in human cancers of the liver, kidney, breast and colon (15-19). Puzianowska-Kuznicka et al. (16) conducted the sequencing of TRβ1 and TRα1 cDNAs. TRβ1 and TRα1 mutations were found in 93.8% and 62.5% of papillary cancer cases, respectively. But no mutations were found in healthy thyroid controls, and only 11.1% and 22.2% of thyroid adenomas had such TRβ1 or TRα1 mutations. Suzuki et al. (20) generated a mouse model (TRβPV/PV mice) of thyroid cancer that harbored a C-terminal 14 amino acid frame-shift mutation in the TRβ gene.
Despite accumulating evidence for a possible role for TR mutants in thyroid tumorigenesis, an elevated rate of thyroid cancers in RTH patients has not yet been observed. It may be that most cases of RTH in humans have heterozygous mutations of TRβ, unlike the TRβPV/PV homozygous mouse model. Other genetic alterations such as BRAF mutation, which is commonly detected the Korean patients with PTC, may also be required to initiate thyroid cancer. Unfortunately, analyses of BRAFV600E mutation or activities of PI3K could not be conducted in our case.
In conclusion, RTH is very rare and easily overlooked, but must be considered in patients who present with goiter and elevated thyroid hormone levels with unsuppressed TSH. Further studies to address the association between thyroid cancer and RTH will shed insight on the molecular and cellular mechanisms of thyroid tumorigenesis.


 XML Download
XML Download