

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multiple births (i.e. twins, triplets and quadruplets) have been associated with increased maternal and fetal morbidity and mortality during pregnancy and delivery including the higher risk for spontaneous abortion, preeclampsia, hydramnios, preterm labor, and maternal hemorrhage (1). Multiple births are associated with a higher frequency of preterm infant (less than 37 weeks of gestation period, GP) and low birth weight infant (LBWI, less than 2,500 gm of birth weight, BW). In addition, the rates of malformations, abnormal growth, and trauma at delivery, are higher than in signleton pregnancies. Therefore, multiple births are considered high risk and require close monitoring and in many cases neonatal intensive care (1-4).
The incidence of spontaneous twinning differs according to country and ethnicity. In general, the frequency is: 1/70 among African Americans, 1/88 among Caucasian Americans , 1/86 among Italians, 1/150 among Greeks, 1/150 among the Japanese, and 1/300 among the Chinese (5). Triplets are estimated to occur in 1 out of [86]2 pregnancies and quadruplets in 1 out of [86]3 pregnancies in the United States (5). Globally, the incidence of multiple births is increasing; since the early 1990s there have been an increased number of pregnancies later in life, and increased use of assisted reproductive technology (ART) such as induction of ovulation and in vitro fertilization (1, 6-9).
The changes in the multiple (twin) pregnancy rate per 1,000 pregnancies have been reviewed in Europe. Investigators from France reported an increase in the twin pregnancy rate to 15.6 in 2008, an 80% increase from 8.9 in 1972 (7, 10). Similar results have been reported from England, where the multiple pregnancy rate was 9.9 in 1975, and increased to 13.6 in 1994, with a marked increase since 1992 (11).
The multiple birth rate (MBR) is defined as the ratio of multiple births per 1,000 live births. A Japanese study reported changes in the MBR from 5.8 in 1975 to 7.0 in 1990, 22.7 in 2005, and 20.5 in 2008 (12). Some Korean studies on the MBR and perinatal morbidity and mortality have been previously reported (13, 14). Hur and Kwon (15) reported a nationwide survey for the first time, using data from the National Satistics of Korea, which includes data on the trends in MBR only from 1981 to 2002 in Korea. In their study, the MBR was maintained within slightly less than 10.0 over a decade from 1981 to 1990. However, it started to increase gradually from the early 1990s, and finally it reached 19.6 in 2002.
On the line of continuity of Hur and Kwon's (15) study, the aim of this study was to focus on the survey of recent trends of multiple births and its consequences on perinatal problems in Korea during the last two decades from 1991 to 2008, to analyze the incidence and the changes in multiple births, the distribution of maternal age, as well as the BW and GP of the infants. The goal was to describe the trends of increasing multiple births, the relationship between maternal age and multiple births, and the incidence of preterm infants and LBWI among the multiple births.
MATERIALS AND METHODS
Data was obtained from the Korean Statistical Information Service (16). The data evaluated included: a) the annual number of multiple biths and MBR, b) maternal age at the time of the birth and the percentage of mothers of advanced-aged, more than 35, c) the distribution of BW and the incidence of LBWI and very low birth weight infants (less than 1,500 g, VLBWI), and d) the distribution of GP and the incidence of preterm infants (subdivided to GP<31, GP: 32-36, and total preterm groups) from 1991 to 2008. All of the results were compared with the same parameters among the total live births during the same time period. Comparison with other countries is also discussed.
RESULTS
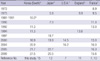
The number of multiple births and MBR in the last two decades
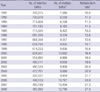
The number of multiple births and the changes in the MBR are shown in Table 1. The total live births decreased. However, the total number of multiple births shows increasing trends. The MBR was 10.0 in 1991, 13.2 in 1995, 16.9 in 2000, 21.7 in 2005, and 27.5 in 2008. There was a 275% increase in the MBR over the last 18 yr. MBR doubling from 10.0 to 20.0 took 12 yr from 1991 to 2003; however, it took only 5 yr to reach 27.5, suggesting a rapid increase in multiple births.
The number of twins and triplets and its rates
The annual number of twins and triplets is shown in Table 2 for the years 2000, 2005, and 2007. The number of triplet births was 123, 69 and 176 in 2000, 2005, and 2007, respectively. The twin birth rate (/1,000 live births) was 16.7 in 2000, 21.6 in 2005 and 26.9 in 2007 and for triplets it was 0.19 in 2000, 0.15 in 2005, and 0.36 in 2007. Both rates show increasing trends.
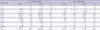
The distribution of maternal age and the percentage of advanced-maternal age
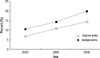
Comparison of the distribution of maternal age between the total live births and multiple births is shown in Table 3. The maternal age for total live births increased from 2000 to 2008. However, the manternal age for multiple births was much higher than for total live births. The percentage of advanced-maternal age for total live births, i.e. more than 35 yr of age, was 6.7% in 2000, 10.6% in 2005, and 14.3% in 2008. For the multiple births, it was 10.5% in 2000, 14.3% in 2005, and 19.8% in 2008, much higher than for total live births (Fig. 1).
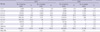
The distribution of BW and the incidence of LBWI and VLBWI
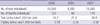
The BW distribution between for total live births and multiple births is shown in Table 4. The BW among multiple births was much lower. The mean BW of total live births was 3.23 kg, and for multiple births it was 2.40 kg in 2008.
The incidence of LBWI among total live births was 3.8%, 4.3%, and 4.9% in 2000, 2005, and 2008, respectively (Fig. 2). For the multiple births, it was 49.2%, 50.3%, 53.0% during the same years. The incidence of VLBWI for multiple births was 2.9%, 4.2%, and 4.7% in 2000, 2005, and 2008, respectively. It was much higher than among total live births. Both showed increasing trends.
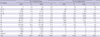
The distribution of GP and the incidence of preterm infants
The distribution of the GP for total live births and multiple births was analyzed (Table 5). The GP was much shorter for the multiple births than the total live births. The incidence of preterm infants among the total live births was 3.8% in 2000, 4.7% in 2005, and 5.5% in 2008, and for the multiple births it was 38.3%, 44.7%, and 51.5% during the same years. These factors showed increasing treands.
The GP was divided into three groups, less than 31 weeks, between 32 and 36 weeks, and total (Fig. 3). The incidence of preterm infants was greater with multiple births than in total live births. These factors also showed increasing trends.
DISCUSSION
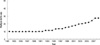
The results of this study (1991-2008) along with those from Hur and Kwon (1981-2002) (15), are shown in Fig. 4. The MBR was maintained within slightly less than 10.0 for a decade from 1981 to 1990. However, it started to increase in 1992 from 11.3 and reached 13.2 in 1995, 16.9 in 2000, 20.0 in 2003, 21.7 in 2005, and 27.5 in 2008. There was a 275% increase in the MBR from 10.0 to 27.5 in the two decades studied. The increase in the MBR in the last 5 yr, was from 20.0 to 27.5, compared to the doubling time of the MBR, in the past, from 10.0 to 20.0, which took almost 12 yr from 1991 to 2003 in Korea.
Numerous factors have been associated with the increase of multiple births, such as social factors, familiar tendency, genetic factors, nutritional factors, fertility, advanced maternal age, and the introduction of ART (1).
Multiple births categorized as twins and triplets, showed that the number of triplets was 123 in 2000, 69 in 2005, and 176 in 2007. The twin birth rate (/1,000 live birth) was 16.7 in 2000, 21.6 in 2005, and 26.9 in 2007, and the triplet birth rate (/1,000 live birth) was 0.19, 0.15, and 0.36 in the same years in Korea. It shows increasing trends. A comparison of the MBR and mutiple (twin) pregnancy rate between Korea and other countries is shown in Table 6. The changes in Korea are consistent with those in Japan, USA, England and France.
Chang et al. (17) reported the first successful ART procedure in Korea in 1986, and it has become widely used gradually from the early 1990s. The Korean Society of Obstetrics and Gynecology reports the annual results through the ART Committee, from their first report titled 'Current status of ART in Korea for 1994' (18) to the latest survey in 2006 (19). The parallel in the incidence of multiple births with the use of ART suggest the importance of the association of ART with multiple births in Korea. In addition, maternal age is another important factor associated with multiple births. The maternal age was found to be higher among multiple births than singleton births, and the percentage of woman considered to be advanced-maternal age was higher among the multiple births. In the results of this study, advanced-maternal age had a frequency of 14.3% among all live births; however, it was 19.8% among the multiple births in Korea in 2008. That is, one out of five mothers among the multiple births were advanced-aged pregnancies. This suggests that advanced-maternal age was one of the factors associated with multiple births. However, Kim et al. (20) reported that the mean age of most women undergoing ART was high; therefore, it is difficult to seperate the two variables (age and ART). We could not determine the number of ART pregnancies accounting for multiple births in the data available for this study. We speculate that studies about the trends of mutiple births by ART in Korea will be required in the next subject.
The incidence of preterm and LBWI is also increasing in Korea. The associated factors include: preterm labor, twinning, ART, social factors, and advanced-maternal age. In the present study, the mean BW was lower and the GP was shorter among multiple births compared to the total live births. These findings suggest that the incidence of preterm and LBWI was much higher among the multiple births. In 2008, LBWI accounted for 53.3% and preterm infants for 51.1% of all multiple births in Korea; that is, half of all multiple births were preterm or LBWI. These findings suggest the need for close monitoring of such pregnancies and deliveries.
In conclusion, the incidence of multiple births and its consequences on perinatal problems (preterm infant, LBWI, and advanced-maternal age at the time of the birth) have been increased steadily over the last two decades in Korea. Such pregnancies, deliveries, and multiple birth infants require close monitoring and care due to the associated risks.


 XML Download
XML Download