

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lymphangioleiomyomatosis (LAM) is a rare disease that occurs mainly in women of reproductive age. The clinical features, including recurrent spontaneous pneumothorax, slow progressive dyspnea, hemoptysis, chylothorax, and chylous ascites, result from progressive cystic lung destruction and accumulation of smooth muscle cells (LAM cells) in the lungs and axial lymphatics (1-4). The primary treatment for LAM consists of hormonal therapy and supportive management, although the response to hormonal therapy has not yet been demonstrated conclusively (4-6).
In 2007, the Korean Interstitial Lung Disease Society had collected data for patients diagnosed with LAM, by a nationwide survey, to establish their demographic, clinical, and radiographic features. This survey showed that the number of new patients with LAM had increased sharply after 2004 (Fig. 1). Therefore, the present study aimed to understand the initial clinical radiological findings, management, and clinical course of patients with LAM in Korea. We also aimed to establish the reason for the recent increase in newly diagnosed patients by comparing the clinical and radiographic features between patients diagnosed with LAM before and after 2004.
MATERIALS AND METHODS
Study population and data collection
We enrolled 63 patients diagnosed with LAM between 1990 and 2007 in Korea. The nationwide survey was performed by collecting the questionnaire-based data sheet between May and September 2007. The data sheet included age at diagnosis, smoking history, previous history of pneumothorax or pleural effusion, presence of tuberous sclerosis complex (TSC) or angiomyolipoma (AML), initial clinical and radiological presentation, comorbidity, initial pulmonary function tests, method of diagnosis, treatment modalities, and survival, and we reviewed retrospectively all items on the data sheets. The diagnosis of LAM was made by lung pathology or typical chest high-resolution computed tomography (HRCT) findings, along with compatible clinical history. Pathologically, LAM was diagnosed in 39 patients (62%), which was based on the results of surgical lung biopsies (n=33), transbronchial lung biopsies (n=4), excisional biopsy of retroperitoneal mass (n=1), or inguinal lymph node biopsy (n=1). In the remaining 24 patients (48%), the diagnosis of LAM was established from typical HRCT findings, which are diffuse, thin-walled cysts scattered in an even distribution throughout the lung fields, with normal intervening lung parenchyma (1).
Survival status was obtained from the death registry of the Korea National Statistical Office as of December 2007. This study was approved by the Institutional Review Board of the Samsung Medical Center (IRB approval number: 2009-12-066).
Statistical analysis
Values are expressed as number (percentile), mean±standard deviation or median (range). Statistical analysis was performed using the unpaired Student's t test for continuous variables and the chi-squared or Fisher's exact test for categorical values, as appropriate. Survival was calculated from the time of diagnosis of LAM until the endpoint (December 2007). Survival probability according to disease duration was estimated by the Kaplan-Meier method. All P values were two-sided, with P<0.05 considered to be statistically significant. Statistical analysis was performed using PASW version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic and clinical characteristics
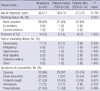
All 63 patients were women, and the mean age at diagnosis was 36 yr (range, 19-65). The age at diagnosis was >40 yr in 35% of the patients. Three patients were ex-smokers and one was a current smoker. The most common past or coexisting disease was pulmonary tuberculosis (11%). AML was found in 21 patients (33%), and eight (13%) had TSC. The main presenting symptom was dyspnea (84%). Pneumothorax was observed in 43% of the patients at diagnosis, and 63% had a previous history of pneumothorax. The median number of patients who experienced at least one episode of pneumothorax was three (range, 1-10).
Twenty-nine patients were diagnosed with LAM before 2004, and the remaining 34 patients were diagnosed after that date. No significant difference existed between the groups for age, history of smoking, and presence of TSC. However, exertional dyspnea was more frequent in the patients diagnosed before than after 2004 (97% vs. 74%; P=0.016; Table 1).
Pulmonary function tests
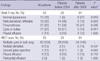
Baseline pulmonary function tests were performed <6 months before or after diagnosis of LAM (Table 2). Spirometry results were normal in 19 of 44 patients whose data were available. The mean values for forced vital capacity (FVC) % predicted, forced expiratory volume in 1 second (FEV1) % predicted (both n=44), total lung capacity (TLC) % predicted (n=24), and diffusing capacity of carbon monoxide (DLCO) % predicted (n=34) were 82.5, 75.8, 99.3, and 74.2, respectively (Table 2). When lung function was compared between patients diagnosed before and after 2004, those diagnosed before 2004 had more severe impairment in FEV1 % predicted (60.3 vs. 85.5, P=0.003), FEV1/FVC ratio (60.5 vs. 83.8, P<0.001), and DLco % predicted (60.9 vs. 80.6, P=0.042; Table 2).
Radiological findings at the time of diagnosis
The main chest radiography finding was the presence of pneumothorax (43%). The reticulonodular infiltration and presence of cysts or bulla upon chest radiography were more common in patients diagnosed before than after 2004 (48% vs. 15%, P=0.004 and 41% vs. 15%, P=0.017), while normal chest radiographic appearance was more common in patients diagnosed after 2004 than before (3% vs. 26%, P=0.017). All patients showed typical, thin-walled parenchymal cysts that were usually distributed homogeneously in both lung fields upon HRCT. Other abnormalities seen with HRCT included nodular densities in 13%, ground-glass opacities in 11%, pleural effusion in 13%, and pericardial effusion in 3% (Table 3).
Treatment modalities and outcome
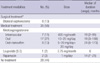
Several medical treatment modalities were tried in 35 patients. Seven of these patients received intramuscular medroxyprogesterone (400 mg/month for a median duration of 19 months), 17 received oral progesterone monotherapy (10-20 mg/day for a median duration of 19 months), and eight received oral progesterone with tamoxifen (median, 24 months). Among the remaining three patients, one was taking gonadotropin-releasing hormone agonist and two were taking rapamycin (Table 4).
Eight patients who received medical treatment underwent oophorectomy. Ten of 21 patients with AML were treated with surgical resection and four with arterial embolization. Of all patients, two patients underwent lung transplantation. One of these patients underwent left lung transplantation and died from chronic graft-versus-host disease at 38 months after transplantation. The other patient is still being followed-up, since April 2007.
Disease course and survival
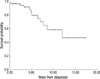
During follow-up, 12 patients died within a median duration of 60 months (1-144 months). Cause of death was attributed to LAM in all patients, directly from respiratory failure (n=11) and lung transplantation morbidity (n=1). The survival probability, evaluated by the Kaplan-Meier method, is shown in Fig. 2. The probability of being alive was 84% at 5 yr and 65% at 8.5 yr after diagnosis.
DISCUSSION
This report provided the clinical and radiological features, and therapeutic modalities of patients with LAM in Korea. The clinical features of Korean patients with LAM do not differ from those reported elsewhere and we also found that the patients recently diagnosed as LAM can be detected at the early stage with mild respiratory symptoms and lung impairment by frequent use of chest CT screening.
Recently, a large number of patients with LAM have been reported (7, 8). These reports have demonstrated that the age range of women with LAM was broader, and normal spirometry at diagnosis was more common than previously reported (2, 9). In addition, the clinical course of these patients with LAM was better than that described earlier, when the majority of patients died from respiratory failure, usually within 10 yr after the apparent onset of the disease (2, 10, 11).
According to the present Korea nationwide survey conducted for patients diagnosed as LAM between 1990 and 2007, the number of LAM patients showed a tendency to increase and it is noticeable that the number of patient newly diagnosed as LAM increased rapidly after 2004 (Fig. 1). In this nationwide survey, although the mean age at diagnosis was similar to that reported previously (2, , 12, 13), the age range (19-65 yr) was as broad as data shown in the National Heart, Lung and Blood Institute (NHLBI) registry of 2006. The most common presenting symptoms were exertional dyspnea and pneumothorax, which was consistent with other studies (8, 12). The prevalence of chylothorax was 20-30% in previous studies (4, 8, 9), but in our study, chylothorax was seen in only one patient at initial diagnosis and in two more during the course of the disease.
Nineteen patients were not available for pulmonary function tests because of dyspnea or pneumothorax at initial diagnosis, but the overall pulmonary function was better when compared to that in previous studies (2, , 13). In patients newly diagnosed with LAM after 2004, FEV1 predicted, FEV1/FVC, and DLco were significantly higher than those in patients diagnosed before 2004. Declines in FEV1 and the FEV1/FVC ratio, which represent progressive obstructive defects, and decreased DLco are sensitive factors for disease progression in LAM (8). Therefore, we suggest that patients diagnosed after 2004 were detected with mild lung impairment, which may mean that it was at an earlier stage compared to those diagnosed before 2004. This was consistent with the finding that clinical symptoms were significantly better, and normal radiographic findings were more frequent in recently diagnosed patients. This earlier detection of LAM in patients with mild symptoms and normal chest radiography might be explained by the widespread and liberal use of CT scanning, which is superior to chest radiography for the assessment of patients with LAM (14). In our study, among 10 patients with normal chest radiographic findings, seven were detected by CT screening (Fig. 3) and three without respiratory symptoms were diagnosed coincidentally for LAM, after undergoing CT scanning for breast cancer, thyroid cancer, or abdominal pain.
In our nationwide survey, 56% of patients received medical therapy and the remainder did not receive it due to rejection of therapy for pregnancy or postmenopausal status, or they had no subjective symptoms. Although the beneficial effect of hormonal manipulation is inconclusive (2, 4, 8), it is the only therapeutic option for LAM. However, a recent nonrandomized, openlabel trial showed that treatment with sirolimus was associated with improvement of lung function in sporadic LAM (15). Additional trials for the relative risks and benefits are needed; however, the use of sirolimus is expected to be promising in the treatment of LAM. Thus, it might be helpful for the treatment of early-detected patients with LAM who show mild symptoms and signs.
In the present study, Kaplan-Meier plots showed survival probabilities of 84% after 5 yr and 65% after 8.5 yr from the time of diagnosis. Previous studies have reported a 3-yr time difference between the time of onset of symptoms and diagnosis, and our result was therefore similar to that of Taylor et al. (4) and Urban et al. (8) who reported 78% and 79% probability of 8.5 yr survival after disease onset.
Our study had several limitations. First, because it was a multicenter retrospective study performed on patients who were diagnosed with LAM over a 18-yr period, treatment protocols were very diverse. And the schedules for following lung function tests were not consistent among hospitals. Thus, the effect of therapeutic interventions on lung function could not be evaluated. In addition, because the follow-up period in patients diagnosed with LAM since 2004 was short, we cannot compare and discuss the natural course of the disease.
In conclusion, our study showed that the clinical features of Korean patients with LAM do not differ from those reported elsewhere. Moreover, we demonstrated that the increment of newly diagnosed patients is the result of increase in detection of the early stage LAM with mild respiratory symptoms and lung impairment by the widespread use of chest CT screening.



 XML Download
XML Download