

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sarcopenia is the age-related decline in lean body mass (1). The prevalence of sarcopenia is about 3-24%, increases with age (2, 3), and is >50% in people older than 80 yr (4, 5). The decline in muscle mass causes a decline in muscle strength and quality (5-7), which lead to frailty and loss of independence in elderly people. Muscle strength is closely related to the absolute quantity of muscle mass, which also declines with aging (8).
Skeletal muscle is a target organ for thyroid hormones, and neuromuscular deficits are well-recognized in hypothyroidism (9, 10). Hyperthyroidism can affect limb muscle mass and strength. In people with overt and subclinical hyperthyroidism, knee flexor and extensor muscle strength and midthigh muscle cross-sectional area are significantly lower compared with values in euthyroid people (11). However, the association between muscle mass or strength and subclinical hypothyroidism has not been reported. Thyroid dysfunction is common in elderly people, and the prevalence of thyroid dysfunction, especially subclinical hypothyroidism, increases with age (12, 13).
In this study, we investigated the prevalence of sarcopenia and the effects of subclinical hypothyroidism on muscle mass, strength, and quality in healthy men and women aged 65 yr or older.
MATERIALS AND METHODS
Subjects
This study was performed as a part of the Korean Longitudinal Study on Health and Aging (KLoSHA) (14). A simple random sample (n=1,118) was drawn from the roster of 61,730 Korean elderly individuals aged ≥65 yr who were residents in Seongnam, Korea, on August 1, 2005. We excluded 217 subjects who had known thyroid disease, regardless of whether they were treated with medication, or had undetermined thyroid function.
We also excluded 96 subjects who had known stroke to exclude its effects on physical disability. Among the 805 subjects enrolled, we selected 797 subjects based on their results on a thyroid function test: 638 had normal thyroid function, 136 were subclinically hypothyroid (SCH), and 23 were overtly hypothyroid (OVH). Measures of thyroid function included the concentrations of serum thyroid-stimulating hormone (TSH) and free thyroxine (fT4), which were measured using a commercial immunoradiometric assay (Abbott, North Chicago, IL, USA). Euthyroidism was defined as concentrations of TSH and fT4 within the normal reference ranges of 0.4-4.1 mU/L and 0.7-1.8 ng/dL, respectively. Subclinical hypothyroidism and overt hypothyroidism were defined as normal and low fT4 concentration, respectively, and elevated TSH were defined as a concentration >4.1 mU/L. All participants were informed fully about the study, and either they or a legal guardian provided written informed consent. The Institutional Review Board of the Seoul National University Bundang Hospital approved the study protocol (B-0508/023-003).
Questionnaires and anthropometric measurements
During the initial visit, all subjects completed a standardized questionnaire designed to evaluate their medical history, which included questions about their history of diabetes mellitus, hypertension, hyperlipidemia, stroke, acute coronary event, and thyroid dysfunction. Current medication profile, smoking and alcohol history, and the presence of body pain were acquired systematically. Height, body weight, waist circumference, and blood pressure were measured. Body mass index was then calculated by determining the ratio between weight and height squared (in kg/m2). Hypertension was defined as a self-reported history of hypertension, use of antihypertensive medication, or blood pressure ≥140/90 mmHg.
Physical activity, performance, and disability were assessed using the physical activity score (PAS) (15), performance-oriented mobility assessment (POMA) (16), short physical performance battery (SPPB) (17), Activity-specific Balance Confidence (ABC) scale (18), the presence of knee pain, and Western Ontario and McMaster Universities (WOMAC) (19). The quality of life was evaluated using the short form 36 (SF36) questionnaire (20).
Laboratory measurement
The plasma fasting and 2-hr postload glucose concentration after ingestion of 75 g oral glucose were measured by the glucose oxidase method using a YSI 2300 STAT glucose analyzer (Yellow Spring Instrument Co., Yellow Springs, Ohio, USA). Total cholesterol, triglyceride, low density lipoprotein cholesterol, high density lipoprotein cholesterol, blood urea nitrogen, and serum creatinine level were measured enzymatically using an autoanalyzer (Hitachi 747, Hitachi, Ltd., Tokyo, Japan) on the same day of the study after the subject had fasted for a minimum of 12-hr. Diabetes was defined as a self-reported history of diabetes or if the subject received antidiabetic treatment, had a fasting plasma glucose concentration ≥7.0 mM/L, or a postload 2-hr glucose concentration ≥11.1 mM/L (21). Metabolic syndrome was defined by the criteria of the National Cholesterol Education Program Adult Treatment Panel III definition using the Asia-Pacific abdominal obesity criteria (waist circumference ≥90 cm in men and ≥80 cm in women) (22).
Muscle mass measurement by computed tomography (CT)
The abdominal adipose tissue areas (visceral fat and subcutaneous fat areas in cm2) and midthigh areas were quantified by a single scout scan with a CT (Somatom Sensation 16, Siemens, Erlangen, Germany). A 5-mm CT slice scan was acquired at the umbilical level to measure the total abdominal and visceral fat areas, and adipose tissue attenuation was then determined by measuring the mean value of all pixels within the range of -190 to -30 Hounsfield units. The scan of the midthigh muscle level was taken at the midthigh, defined as the midpoint from the inguinal crease to the proximal pole of the patella.
Muscle mass measurement by dual energy X-ray absorptiometry (DXA)
Appendicular skeletal muscle mass (ASM) was measured by DXA (Lunar Corporation, Madison, WI, USA). We used 2 definitions for sarcopenia. One was the ASM divided by height squared (ASM/Ht2, expressed as kg/m2) proposed by Baumgartner et al. (4). The other was ASM as a percentage of body (ASM/Wt expressed as a percentage), which was modified from the study of Janssen et al. (23). Sarcopenia was defined as <1 standard deviation (SD) below the sex-specific mean for a young reference group. The cutoff point for sarcopenia was 7.09 kg/m2 in men and 5.27 kg/m2 in women using ASM/Ht2. For ASM/Wt, the cutoff was 29.9% in men and 25.1% in women. The sex-specific young reference group included 32 healthy men (mean age, 28.4±3.1 yr) and 38 women (mean age, 26.3±2.6 yr). All scans were obtained by one certified technician. Total and leg lean body mass, total fat mass, and total body bone mineral content were measured in kilograms.
Muscle strength and muscle quality measurements
Maximum isometric knee extension and flexion strength were measured as peak force (in kilograms) on a digital force gauge fixed to a stand. Muscle strength was measured during knee extension and flexion using an isokinetic dynamometer (Biodex Isokinetic Tester, Biodex Medical Systems, Inc., Shirley, NY, USA). Force was measured in both legs unless contraindicated by pain or a history of joint replacement. We obtained total work from the sum of the total area under all the torque curves in the 20 test repetitions. Muscle quality was assessed by the ratio of peak torque or total work to the leg lean mass obtained by DXA (5) or the midthigh muscle area obtained by CT.
Statistical analysis
The data are presented as means±SD or numbers (percentages) separately for men and women. Student's t test and a chi-square test were used to compare variables between SCH subjects and euthyroid subjects. Analysis of variance (ANOVA) was used to compare the 3 groups (euthyroid, SCH, and OVH). P<0.05 was considered significant. Binary logistic and multiple regression analyses were used to examine the relationships between thyroid status, sarcopenia, muscle mass, strength, and quality.
RESULTS
Anthropometric and laboratory characteristics of the subjects
The men included 280 euthyroid, 61 SCH, and 7 OVH subjects. Their mean fT4 and TSH concentrations differed significantly between groups (fT4, 1.26±0.25 in euthyroid, 1.24±0.24 in SCH, 0.63±0.07 in OVH subjects; P<0.001; TSH, 2.25±0.90 in euthyroid, 6.17±1.98 in SCH, and 16.91±18.34 in OVH subjects; P<0.001). The men's anthropometric and metabolic characteristics including body mass index, waist circumference, blood pressure, glucose and lipid profiles, and muscle enzyme levels did not differ between groups. Use of alcohol, smoking, past medical history of diabetes, hypertension, or an acute coronary event, and the prevalence of metabolic syndrome also did not differ between groups (data not shown).
The women showed similar characteristics as the men; there were 358 euthyroid, 75 SCH, and 15 OVH subjects. Their mean fT4 levels were 1.20±0.25 in euthyroid, 1.14±0.27 in SCH, and 0.59±0.12 in OVH (P<0.001). The TSH levels were 2.31±0.91 in euthyroid, 6.60±3.03 in SCH, and 26.29±45.64 in OVH subjects (P<0.001). Only the mean age of the OVH group (82.4±8.2 yr) was significantly higher than in the other groups (euthyroid, 76.1±9.2; SCH, 74.6±8.0) (P=0.008). All other parameters did not differ significantly between groups (data not shown).
The effects of subclinical hypothyroidism on muscle mass or sarcopenia
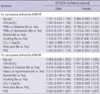
Muscle mass measured by DXA or CT did not differ between euthyroid subjects and SCH subjects in men or women (Table 1). Muscle mass tended to be lower in OVH subjects (men, 44.9±4.8 kg; women, 33.0±4.6 kg) than in euthyroid subjects (men, 47.6±5.0 kg; women, 34.7±6.5 kg) and SCH subjects (men, 47.3±4.8 kg; women, 33.3±3.0 kg), but these differences were not significant, possibly because of the small number of OVH subjects. Fat mass, fat area by CT, and midthigh muscle area by CT did not differ between groups. The prevalence of sarcopenia defined as ASM/Ht2 was 34.9% in men and 9.6% in women; the prevalence of sarcopenia defined as ASM/Wt was 38.8% in men and 50% in women.
When analyzed according to thyroid hormonal status, the prevalence of sarcopenia by both definitions did not differ between the euthyroid, SCH, and OVH men (Table 1). Among women, the prevalence also did not differ between the euthyroid and SCH groups when defined as ASM/Wt (49.3% vs. 65.0%); however, when defined as ASM/Ht2, the prevalence was higher in SCH than in euthyroid women (22.5% vs. 9.4%).
We performed multivariate analysis to investigate further the variables associated with sarcopenia. Age, the presence of diabetes, alcohol use, and smoking were risk factors for sarcopenia (Table 2). Subclinical hypothyroidism and increased TSH levels were not associated with sarcopenia. All the other indexes of leg muscle mass, muscle strength, and muscle quality were not associated with thyroid dysfunction in both men and women (data not shown). Taken together, these data suggest that subclinical hypothyroidism has no additional harmful influence on muscle mass or sarcopenia in elderly subjects.
The effects of subclinical hypothyroidism on muscle strength and muscle quality
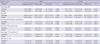
Table 3 shows the peak torque and total work (representing muscle strength) of the dominant leg measured using an isokinetic dynamometer. Muscle strength measured during flexion or extension did not differ between euthyroid and SCH subjects. Muscle strength showed a nonsignificant tendency to be lower in OVH subjects than in euthyroid and SCH subjects. Similar results were observed for the indexes of muscle quality (leg peak torque or total work divided by DXA leg lean or CT midthigh muscle area) in euthyroid and SCH subjects. Muscle quality by CT area was lower in OVH subjects than in euthyroid and SCH subjects, with borderline significance. When we compared these indexes of muscle strength and muscle quality between the right and left legs, the results were similar between the dominant and non-dominant legs (data not shown).
The effects of subclinical hypothyroidism on physical activities or performances
To determine whether thyroid functional status was associated with physical performance, the presence of disability, and quality of life in these subjects, we used the PAS, ABC scale, POMA, and SPPB to represent physical performance, and the presence of knee pain and the WOMAC to evaluate the presence of disability. Quality of life was evaluated using the SF36 questionnaire. The scores on these scales did not differ between thyroid function groups in men and women (data not shown).
DISCUSSION
The number of elderly people is increasing markedly worldwide. Aging is associated with a decrease in lean body mass and increase in fat mass (1). Sarcopenia affects muscle mass, strength, and quality, and these changes are associated with physical disability, morbidity, and mortality. Sarcopenia is of considerable clinical importance in elderly people.
Sarcopenic women have 3.6-times higher rates of disability and sarcopenic men have 4.1-times higher rates compared with people with normal muscle mass (4). The causes of sarcopenia are diverse. Neuronal loss and changes in hormones such as sex hormones, growth hormone, and insulin adversely affect muscle mass. Diabetes mellitus is associated with severe muscle wasting, and the risk of insulin resistance increases with aging, fat mass, and physical inactivity (24). Baumgartner et al. (25) reported that muscle mass is significantly associated with heart disease in older men and with total fat mass in older women.
The prevalence of thyroid dysfunction, especially subclinical hypothyroidism, is increasing because of the increase in routine screening of thyroid function. The prevalence of subclinical hypothyroidism also increases with age (13) and now affects 5-10% of the general population and up to 20% of older women (26, 27). Skeletal muscle is a target organ for thyroid hormones (9, 10). Both hypothyroidism and hyperthyroidism can affect limb muscle mass and muscle strength. Treatment of hypothyroidism with thyroid hormone improves skeletal muscle function (28). In SCH and OVH subjects, knee flexor and extensor muscle strength and midthigh muscle cross-sectional area are significantly lower than the values in euthyroid subjects (11). However, the association between muscle mass or muscle strength and subclinical hypothyroidism has not been reported until now. We evaluated these associations for the first time, and we conclude that muscle mass, the prevalence of sarcopenia, muscle strength, and muscle quality are not affected by mild thyroid dysfunction in elderly people.
The female SCH subjects in our study had a higher prevalence of sarcopenia defined as ASM/Ht2 than did the euthyroid subjects (22.5% vs. 9.4%). To rule out the effects of other risk factors for sarcopenia, we excluded subjects with history of stroke because it is the most well-known risk factor associated with loss of muscle mass and muscle function (29, 30). We also adjusted for other covariates, such as blood glucose and lipid levels, in the multivariate analysis and found no effect of subclinical hypothyroidism on muscle function and sarcopenia. However, in the correlation analysis (data not shown), total muscle mass, and muscle areas measured by CT correlated more strongly with ASM/Ht2 (muscle mass, r=0.356, P<0.001; midthigh CT muscle area, r=0.330, P<0.001) than with ASM/Wt (muscle mass, r=-0.051, P=0.489; midthigh CT muscle area, r=0.108, P=0.229). Thus, although the statistical significance disappeared after multivariate analysis, the possible relationship between sarcopenia and SCH, at least in elderly women, cannot be ruled out completely.
Muscle mass, strength, and quality did not differ between euthyroid, SCH, and OVH subjects within either sex. Indices of physical performance, disability, and quality of life did not differ between SCH and euthyroid subjects. Even after the multivariate analysis including age, diabetes and hypertension, history of acute coronary event, alcohol, smoking, presence of pain, physical activity score and lipid profile, TSH level was not associated with muscle mass, muscle strength, or muscle quality. We found no definite evidence of an association between subclinical hypothyroidism and muscle mass or function in this group of older people study.
Our data showing no relationship between hypothyroidism and anthropometric and laboratory characteristics, muscle mass, strength, and quality contrast with other reports (11, 28). This difference may relate to the small number of enrolled OVH subjects (n=23) and even smaller numbers after dividing the group by sex (7 men, 16 women). However, muscle strength and quality showed a borderline significant tendency to be lower in the OVH group, suggesting that hypothyroidism affects muscle function in elderly people. It is also possible that, in all elderly subjects, the effects of aging itself are so large that they mask any adverse effects on muscle caused by overt or subclinical hypothyroidism.
In conclusion, subclinical hypothyroidism has little influences on muscle mass, strength, and quality, and may not be associated with sarcopenia in elderly people.

 XML Download
XML Download