

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Metabolic syndrome (MetS) has an age-adjusted prevalence rate of 24% in adults in the USA and 11-19% in Korea (1-4). It is characterized by a cluster of clinical features that include abdominal obesity, insulin resistance, hyperglycemia, hypertension, and dyslipidemia. These risk factors act synergistically to increase the risk of adverse cardiovascular events including coronary artery disease and congestive heart failure, and are associated with high cardiovascular morbidity and mortality (5, 6). The progressive addition of MetS risk factors such as obesity, diabetes, and/or dyslipidemia is associated with increased left ventricular (LV) mass, an effect which is independent of hypertension. The effects of MetS on cardiovascular structure and function are not well characterized (7). We therefore investigated the relation between MetS and LV geometry and function, carotid intimamedia thickness (IMT), and arterial stiffness using a sample from the Korean general population.
MATERIALS AND METHODS
Study population
The ARIRANG study (Atherosclerosis RIsk of a Rural Area koreaN General population) is an ongoing study of cardiovascular and metabolic risk factors that is being conducted in the rural area of Wonju, Gangwon-do, Korea. The ARIRANG study was approved by the Ethics Committee of the Wonju Christian Hospital, Wonju College of Medicine, Yonsei University (Wonju, Gangwon-do, Korea, Approval number: CR105024), and written informed consent was obtained from all study participants. In the present study, we investigated a total of 702 adults from the ARIRANG cohort who had all previously undergone complete echocardiography assessment and measurement of IMT and pulse wave velocity (PWV). For the present study, all participants underwent a complete cardiovascular evaluation following 8 hr of fasting, which included: 1) history, physical examination, and anthropometric analysis; 2) measurement of heart rate and blood pressure (BP, measured after 10 min resting in a sitting position, was expressed as the average of three consecutive measurements taken from each arm); 3) measurement of fasting blood glucose and insulin levels (in subjects not receiving insulin and/or oral hypoglycemic agents); and 4) measurement of fasting plasma lipids (i.e., concentrations of triglyceride, high-density lipoprotein cholesterol [HDL-C], total cholesterol, and low-density lipoprotein cholesterol [LDL-C]). A diagnosis of MetS was assigned according to the amended National Cholesterol Education Program's Adult Treatment Panel III (ATP-III) Guidelines and using the South Asian-specific value for waist circumference. MetS was diagnosed in individuals meeting three or more of the following criteria: (a) increased waist circumference (≥90 cm in males or ≥80 cm in females); (b) increased fasting triglyceride level (≥150 mg/dL); (c) high BP (≥130/≥85 mmHg) or receiving antihypertensive therapy; (d) decreased HDL-C level (<40 mg/dL in males or <50 mg/dL in females) or receiving specific treatment for this lipid abnormality; and (e) impaired fasting glucose level (≥110 mg/dL) (1, 4).
Echocardiography
Echocardiography was performed using the harmonic imaging mode by use of a 3-MHz transducer and commercial ultrasound system (Vivid-7; General Electric-Vingmed, Milwaukee, WI, USA). LV internal dimensions, LV wall thickness, and LV ejection fraction (LVEF, by modified Simpson's rule) were measured according to published recommendations (8). LV mass was calculated as recommended by the American Society of Echocardiography using the equation: LV mass =1.04×([PW+VS+LVDd]3×[LVDd]3)×0.8+0.6, where PW is the M-mode posterior wall thickness of the LV, VS is the M-mode interventricular septal thickness, and LVDd is the M-mode LV dimension with the short axis view at end-diastole (9). Allometric height-based adjustments were used since height2.7 has been reported to offer the most accurate estimation of LV hypertrophy and risk factors for pathological changes in heart structure, particularly in obese subjects (10). Relative wall thickness (RWT), which increases with concentric remodeling and concentric hypertrophy, was calculated as 2×PW/LVDd. The left atrial (LA) dimension was measured by 2D-guided M-mode echocardiography using the parasternal short-axis view at the base of the heart, as recommended by the American Society of Echocardiography (11). Three LA dimensions were used to calculate the LA volume as an ellipse using the formula: LA volume=π/6 (SA1 • SA2 • LA), where SA1=the M-mode LA dimension, and SA2 and LA are measurements of the short- and long-axis with the apical four-chamber view at ventricular end-systole, respectively (12). The LA volume index was calculated by dividing the LA volume by the body surface area (BSA, m2).
Transmitral inflow velocities were measured using Pulsed-Wave Doppler (PWD) and the apical 4-chamber view, with the sample volume placed at the mitral valve leaflet tips (13). Measurements of the transmitral early diastolic (E-wave) and atrial (A-wave) velocities were taken in order to calculate the E/A ratio and E-wave deceleration time (13). Tissue Doppler imaging (TDI) and the apical 4-chamber view were used to measure the LV myocardial velocities, with the sample volume placed at the septal mitral annulus (13, 14). Measurements included the early diastolic velocity (E') and late diastolic velocity (A'). The E/E' ratio was then calculated (15).
Measurement of carotid IMT and PWV
Measurement was performed using a validated procedure, as described previously (16). An ultrasound system (Vivid-7; General Electric-Vingmed) and a phased array 12-MHz transducer were used to obtain a high-resolution B-mode ultrasound view of the far wall of the common carotid artery. The common carotid arteries were explored, starting from a position 1 cm below the flow divider and between the internal and external carotid arteries. Measurements were taken by tracing the leading edge of the lumen-intima and the media-adventitia interfaces in plaque-free areas.
PWVs were measured using an automatic waveform analyzer (PP-1000, Hanbyul Meditech, Jeonju, Korea). This provides regional PWV values using simultaneous electrocardiographic, phonographic, and pulse wave measurements from four different arterial sites (carotid, femoral, radial, and dorsalis pedis). The PWV was then calculated from the pulse transit time and the distance travelled by the pulse between the two recording sites: PWV=Distance (meters)/Transit time (seconds). Surface distances for the measurement of the PWV were calculated from the subject's height and from anthropomorphic data from the Korean population. Three different PWV values were calculated: aortic, heart-to-radial, and femoral-to-ankle. The aortic PWV represents the velocity between the carotid artery and the femoral artery. The heart-to-radial PWV (hrPWV) and the femoral-to-ankle PWV (faPWV) were calculated on the basis of the carotid- radial and the femoral-dorsalis pedis transit times, respectively.
Statistical analysis
Statistical analyses were performed using SPSS 11.0.1 software (SPSS Inc., Chicago, IL, USA). Males and females were analyzed separately since sex is known to have an important effect. The study cohort was divided into three groups according to the number of MetS criteria present: Absent (0 criteria), Pre-MetS (1-2 criteria), and MetS (≥3 criteria). The data are presented as mean±standard deviation in the case of continuous variables and as proportions in the case of categorical variables. Chi-square statistical analysis was used to determine differences in categorical variables between the three groups. Analysis of variance (ANOVA) was used to determine differences in continuous variables between the three groups. P values for the comparison of echocardiographic parameters of cardiac geometry and function across the three groups were based on analysis of covariance (ANCOVA), adjusted for age and BP. The comparisons of IMT and PWV were analyzed by ANCOVA, and adjusted for age, BP, and smoking habits. Given the co-linearity of the components of the metabolic syndrome, the effect sizes of the components of the metabolic syndrome on cardiac geometry, IMT and PWV adjusted for age and compared using single linear regression analysis. A two-sided P<0.05 was considered statistically significant.
RESULTS
Characteristics of the study population
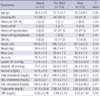
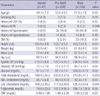
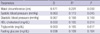
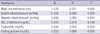
The prevalence of MetS was 38.6% (36.6% of males and 40.0% of females, P=0.20). The demographic and clinical characteristics of the 702 subjects (mean age, 55.5±8.5 yr; 41% male) are reported separately for each sex, according to the number of MetS criteria present (Tables 1, 2). Due to the sampling effect, the values of the MetS components (waist circumference, BP, fasting glucose, triglyceride level), weight, and hip circumference measurements were found to increase across the three groups, while the HDL-cholesterol levels decreased across the three groups. In female subjects, a stepwise increase in the level of total cholesterol and LDL cholesterol, and in the prevalence of cardiovascular disease (cerebrovascular accident, myocardial infarction and hypertension), was observed across the three groups. No significant differences in these factors were observed in male subjects.
Cardiac geometry and function
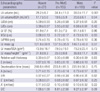
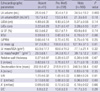
The mean LVEF was 62.7±7.6% and the mean LV mass was 124.5±38.9 g. LVEF was lower in males (61.3±7.7% vs. 63.7±7.4%, P<0.001). LV mass and LV mass/BSA were significantly higher in males (139.4±39.1 g vs. 114.1±35.3 g, 78.6±20.6 g/m2 vs. 72.0±20.3 g/m2, P<0.001). No sex difference was observed for LV mass/height2.7 (35.4±10.0 g/m2.7 vs. 36.0±11.6 g/m2.7, P=0.49). E/E' was significantly lower in males (8.9±2.7 vs. 10.9±3.2, P<0.001). The LA volume index was similar in both sexes. In males, the LA volume and LA volume index showed a stepwise increase across the three groups, but no inter-group differences were observed for the other echocardiographic parameters (Table 3). In females, LV mass, LV mass/height2.7, and LA volume increased in a stepwise manner across the three groups; no inter-group differences were observed for LVEF. LVDd and RWT showed a tendency to increase across the three groups, but these differences did not achieve statistical significance. The E' showed a stepwise decrease across the three groups, and deceleration time increased across the three groups. Since the A wave velocity showed a tendency to increase and the E wave velocity showed a tendency to decrease, the E/A ratio decreased in a stepwise manner across the three groups (Table 4). In comparing the effect size of each component of the metabolic syndrome, waist circumference was found to have the most powerful effect on both LV mass/height2.7 and deceleration time in female subjects (Tables 5, 6).
Carotid IMT and PWV
IMT ranged from 0.22 to 1.75 mm, with a mean of 0.62 mm and a standard deviation (S.D.) of 0.15 mm, and was similar in both sexes. The coefficient of variation of IMT was 24.1%. A significant positive correlation was observed between IMT and systolic blood pressure (r=0.098, P=0.01) and age (r=0.236, P=0.00), irrespective of smoking status. IMT was also found to be significantly correlated with hrPWV (r=0.098, P=0.03) and faPWV (r=0.093, P=0.04), but not with aortic PWV. The mean aortic PWV was 7.66±1.26 m/sec (coefficient of variation=16.4%), hrPWV was 8.12±1.07 m/sec (coefficient of variation=13.0%), and faPWV was 10.15±1.35 m/sec (coefficient of variation=13.3%). PWV was significantly higher in males (Aortic PWV, 8.05±1.25 m/sec vs. 7.38±1.2 m/sec; hrPWV, 8.61±1.03 m/sec vs. 7.77±0.95 m/sec; faPWV, 10.34±1.30 m/sec vs. 10.01±1.36 m/sec, P<0.01). Aortic PWV and faPWV were significantly correlated with systolic and diastolic blood pressure and age; hrPWV was correlated with BP, but not with age. Significant differences were observed for all regional PWVs in relation to smoking status (non-smoker, exsmoker, current smoker).
In males, IMT was significantly higher in the MetS group compared with the pre-MetS group (P=0.01). All regional PWVs were similar across the three groups (Figs. 1, 2).
In females, IMT was significantly higher in MetS group compared with the two other groups (Fig. 1). Aortic PWV increased in a stepwise manner across the three groups (6.97±0.97 m/sec, 7.16±1.13 m/sec, 7.74±1.26 m/sec, P=0.049) (Fig. 3). hrPWV and faPWV showed a tendency to increase in a stepwise manner across the three groups, but these differences did not achieve statistical significance (Fig. 3). In comparing the effect size of each component of the metabolic syndrome, waist circumference was found to have the largest effect on IMT (Table 7).
DISCUSSION
The present study evaluated echocardiographic measurements of LV geometry and function, IMT and PWV assessment of arterial stiffness in a cross sectional cohort of subjects grouped according to the number of MetS criteria present. This study clearly demonstrated a sex specific relationship between MetS and cardiovascular function and geometry. The fact that the ANCOVA model was used reduces the likelihood that this finding was an artifact of covariance (age, BP, or smoking). In females, we found that: 1) LVEF, which reflects LV systolic function, was within normal limits in all three groups, 2) RWT results were similar in all three groups, while LV mass and LV mass/height2.7 increased progressively across the three groups, 3) E/A and deceleration time, which reflects LV diastolic function, showed progressive impairment across the three groups after adjustment for age and BP, and 4) aortic PWV increased progressively across the three groups after adjustment for age, BP and smoking status. In males, no differences were found across the three groups, except in LA volume index and IMT. The results of this study suggest that an increase in the number of MetS criteria is associated, in an independent manner, with subclinical eccentric LV hypertrophy, diastolic dysfunction, and increased arterial stiffness, irrespective of age and BP. The effects of MetS were found to be pronounced in females, but not in males. These findings did not change when subjects with diabetes and hypertension were excluded (data not shown). When LV mass was indexed for body surface area (a normalization that minimizes the effect of obesity since body weight is included in its computation), metabolic risk factors showed no significant effects. This finding strongly confirms that obesity, when present, is the feature that tracks the cumulative effect of the other risk factors (hypercholesterolemia and diabetes).
Although several recent studies have reported impaired LV diastolic function in MetS patients, consensus is still lacking on the effect of MetS on cardiac function and geometry. In the Strong Heart Study, MetS was found to be associated with reduced LV systolic and diastolic function and LV dimensions, while LV mass and RWT were found to be higher in the MetS group (17). In contrast, Grandi et al. (18) found that only LV diastolic function was reduced in MetS, and that LV systolic function was normal in clinically hypertensive non-diabetic subjects. They also reported that both LV mass and relative wall thickness were significantly increased in the MetS group, but that LV dimensions were similar in both groups. Mule et al. (19) reported that MetS has a deleterious effect on hypertension-related target organ damage. They observed increased LV mass, RWT, and deceleration times in hypertensive subjects with MetS compared with a hypertensive cohort without MetS. In a population-based study, Sundst-rom et al. (20) demonstrated a strong correlation between MetS and left ventricular mass and relative wall thickness, a correlation which was independent of blood pressure status. Only a few previous studies of the impact of MetS on LV mass have conducted separate analyses for males and females, and these studies have reported conflicting findings. Schillaci et al. (21) found that MetS had a more pronounced effect on LV hypertrophy and function in females. Our results support the hypothesis that MetS is associated with LV diastolic dysfunction in females only, even in subjects without LV systolic dysfunction, and irrespective of BP status. However, in the present study, changes in LV geometry tended toward eccentric hypertrophy, and waist circumference was found to have the most significant effect on left ventricular functional and geometric change.
In the present study, MetS was associated with increased carotid IMT and aortic PWV, and this effect was independent of age, BP, and smoking status, particularly in females. In females, hrPWV and faPWV showed a tendency to increase in a stepwise manner across the three groups, but these differences did not achieve statistical significance. This suggests that the cluster of MetS components may interact synergistically to increase arterial stiffness, particularly in females. Several previous studies have reported that the grouping of insulin resistance syndrome components is associated with excessive carotid IMT, beyond a level attributable to an additive effect, and that MetS was independently associated with carotid IMT and arterial stiffness (22, 23). However, most of the studies that have investigated associations with MetS and its components have focused on one specific arterial segment, such as the aorta, brachial-ankle segment, or the lower limb, or alternatively, one arterial site such as the brachial and (more frequently) the carotid artery, and their results have been conflicting. There have been few studies of sex-specific MetS effects on arterial stiffness. Schillaci et al. (24) demonstrated that MetS was independently associated with higher aortic velocity, but not with higher upper limb pulse wave velocity. Ferreira et al. (25) reported that stiffness in the femoral arteries was higher than that in the carotid arteries. Other studies have evaluated central and peripheral arterial segments and reported that MetS is associated with increased central and peripheral arterial stiffness in females (26). The present study showed an association between MetS and aortic PWV in females, but these findings did not reach statistical significance. Further studies are required to demonstrate the relative impact of MetS on PWV in differing arterial regions.
The mechanism underlying the influence of sex on the association between MetS and LV geometry and function, arterial stiffness, and structural change remains unknown. It will be necessary to conduct further studies in order to elucidate the nature of this sex-specific effect.
The present study has important limitations. Its cross-sectional design precludes the performance of outcome analyses. The sample size was relatively small, especially for the group with no MetS components. Ambulatory BP measurements, which have been shown to be more predictive of hypertensive end-organ damage, were not performed. Although PWV may vary according to the time of day, these variables were consistently measured in the morning.
In conclusion, clustering of MetS components is independently associated with subclinical eccentric LV hypertrophy, diastolic dysfunction, and increased aortic wall stiffness, particularly in females, irrespective of age and BP status. Waist circumference has the most powerful influence on LV geometry and function and IMT.




 XML Download
XML Download