

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Squamous cell carcinoma of the head and neck (SCCHN) is the fifth most common cancer worldwide and accounts for 3.5% of the cancers registered in Korea during 2001 (1). SCCHN is believed to be induced by environmental and host factors. The main causative environmental factors are tobacco or alcohol use, viral infection, nutritional deficit, mineral inhalation and history of radiation exposure (2, 3). Accumulating evidence has shown that genetic polymorphisms influence the risk of environmental carcinogenesis (4-6), and that genetic susceptibility plays an important role in the development of SCCHN. Therefore, it has been suggested that susceptibility to SCCHN may be due to genetic polymorphisms in genes controlling carcinogen metabolism, repair of DNA damage, or genes related to cancer development, such as various cytokine genes and cyclooxygenase-2 (COX-2) (7-11).
Cyclooxygenase (COX) is a key enzyme that mediates the conversion of free arachidonic acid to prostaglandin. COX consists of two isoforms, COX-1 and COX-2 (12). COX-1 is constitutively expressed in most tissues for physiologic homeostasis. In comparison, COX-2 is rapidly activated by growth factors and mitogen and plays an important role in inflammation and tumor development (13).
Interleukin-10 (IL-10) is an important immunoregulatory cytokine in humans that is secreted by helper T-cells and synthesized by activated macrophages (14). IL-10 has the inhibitory properties of inflammatory cytokines like interferon gamma, IL-2, and IL-3, which are produced by macrophages and helper T-cells (14). The functions of IL-10 in humans range from the anti-inflammatory activity associated with auto-immune disease to tumor development and growth, as demonstrated by reports of increased IL-10 levels in cancer patients (14, 15).
Recently, several polymorphisms in COX-2 and IL-10 have been found to be associated with inflammation and tumor development. It is also thought that these polymorphisms may cause the differential expression of these genes, resulting in susceptibility to cancer development. Many studies have linked COX-2 and IL-10 genetic polymorphisms with various types of carcinoma (16, 17), but the COX-2 and IL-10 genetic polymorphisms have not been studied in cases of SCCHN in a Korean sample. In this study, we investigated the frequencies of single nucleotide polymorphisms (SNPs) in COX-2 and IL-10 between SCCHN patients and controls in a Korean sample and evaluated the effect of the COX-2 and IL-10 polymorphisms on the risk of SCCHN.
MATERIALS AND METHODS
Study population
For our hospital-based case-control study, we recruited subjects from the Department of Otolaryngology, Hanyang University Hospital, Seoul, Korea from 1997 to 2004. The case group consisted of 290 cases with pathologically-verified SCCHN. The cases were newly-diagnosed SCCHN patients, with the following primary sites: larynx (n=148), oral cavity (n=69), oropharynx (n=39), hypopharynx (n=39) and other (n=4). For the control group, we enrolled 358 hospital-based chronic otitis media, chronic sinusitis, and chronic tonsillitis patients. Cases and controls with a history of previous malignant disease or a genetic disease were excluded. The mean age of the case group was 62.6 yr (range, 28-90), with 252 males and 38 females. The mean age of the control group was 38.8 yr (range, 21-76), with 339 males and 19 females. All patients and controls were of Korean ethnicity. All participants provided informed consent. The Institutional Review Board of College of Medicine, Hanyang University approved the study protocol (December 15, 2008). Peripheral blood specimens were collected from all the subjects and stored at -80℃ before DNA isolation.
Genotyping
We performed DNA extraction from peripheral blood using the Wizard™ Genomic DNA purification kit (Promega, Madison, WI, USA). We analyzed three SNPs of COX-2 (-1329A>G, +1266C>T, and +6365T>C) and three SNPs of IL-10 (-1082A>G, +920T>G, and +3917T>C). We performed single base extension (SBE) for genetic analysis of all SNPs, except for COX-2 +6365T>C. The polymerase chain reactions (PCR) included primers (1.25 pM each), 5 ng genomic DNA, 250 µM dNTPs and 0.15 U Taq DNA polymerase (Applied Biosystems, Foster City, CA, USA) and were run using the GeneAmp PCR System 9700 Thermocycler (Applied Biosystems). The primers used are listed in Table 1. Using the SNaPshot ddNTP primer extension kit (Applied Biosystems), we performed the primer extension reaction. To clean-up the primer extension reaction products, 1 U shrimp alkaline phosphatase (Amersham Life Science, Cleveland, Ohio, USA) was added to the reaction mixture, and the mixture was incubated at 37℃ for one hour, followed by 15 min at 72℃ for enzyme inactivation. We added the amplified material and Genescan 120Liz size-standard solution (Applied Biosystems) in Hi-Di formamide (Applied Biosystems) and incubated the reaction at 95℃ for five minutes, followed by incubation on ice for five minutes. Electrophoresis was performed using the reaction mixture with an ABI Prism 3100 Genetic Analyzer (Applied Biosystems). We used ABI Prism GeneScan and Genotyper to perform the genetic analyses.
The analysis of the COX-2 +6365T>C SNP was performed using the TaqMan assay. The forward and reverse primers were: 5'-GCATCTTCCATGATGCATTAGAAGTAAC-3', 5'-GCACTGATACCTGTTTTTGTTTGATGA-3'. The probe for the wildtype (T allele) was 5'-AAGTACTTTTGGTTATTTTT-3'. The 5' end was conjugated with VIC™ fluorescent dye and the 3' end was conjugated with TAMRA™ quencher dye. The probe for the mutant type (C allele) was 5'-ACTTTTGGTCATTTTT-3', with the 5' end bound to FAM™ fluorescent dye and the 3' end bound to TAMRA™ quencher dye. PCR was performed in a 5 µL reaction that consisted of a mixture of TaqMan universal PCR master mix (Applied Biosystems), UNG, primers (900 µM), probe (200 nM) and genomic DNA (20 µg). The PCR reaction conditions were as follows: 50℃ for two minutes, 95℃ for ten minutes and then 15 sec denaturing, final annealing and extension at 60℃ for one minute, for 40 amplification cycles. The TaqMan assay plate was transferred to a Prism 9700HT instrument and genetic analysis was performed by measuring the fluorescence level in each well.
Statistical analyses
Statistical verification of the associations of COX-2 and IL-10 genetic polymorphisms with SCCHN and with the normal control group was performed using a chi square test. The odds ratios (OR) and 95% confidence intervals were obtained using a logistic regression model. All statistical analyses were performed using the SPSS statistical package (SPSS, version 12.0, Inc., Chicago, IL, USA).
RESULTS
COX-2 polymorphisms
For the COX-2 -1329A>G SNP (genotyping was available in 621 of 648 subjects), the frequency of variant allele G was 44.2% and heterozygosity was 46.8%. The frequency of the COX-2 genotypes, -1329 AA, AG and GG, were 31.7%, 46.9%, 21.4% in the case group and 32.9%, 46.9%, and 20.3% in the control group respectively. The odds ratio and respective 95% confidence intervals for the genotype AG and GG in reference to AA were 1.08 (0.78-1.49) and 1.00 (0.61-1.65), respectively. For the COX-2 +1266C>T SNP (genotyping was available in 621 of 648 subjects), the frequency of variant allele T was 0.7% and the heterozygosity was 1.4%. The frequency of the COX-2 genotypes, +1266 CC, CT, and TT, were 97.8%, 1.8%, and 0.4% in the case group and 98.9%, 1.1%, and 0% in the control group, respectively. The relative risk of CT to CC was 1.11 (0.21-5.99). For the COX-2 +6365T>C SNP (genotyping was available in 587 of 648 subjects), the frequency of variant allele C was 20.8% and heterozygosity was 33.2%. The frequency of the COX-2 genotypes, +6365 TT, TC, and CC, were 64.7%, 32.1%, and 3.2% in the case group and 61.2%, 34%, and 4.7% in the control group, respectively. The relative risks of TC and CC to TT were 1.01 (0.55-1.84), and 0.78 (0.49-1.26), respectively. We found no statistical significance in our analyses (Table 2).
COX-2 haplotypes
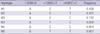
We identified six haplotypes (GCT, ACT, ACC, ATC, GCC, GTT) for COX-2 -1329A>G, +1266C>T, and +6365T>C and analyzed the three most common haplotypes, which we abbreviated as ht1 (GCT), ht2 (ACT), and ht3 (ACC) (Table 3). The haplotype distributions are summarized in Table 4.
The frequencies of ht3 -/-, +/-, and +/+ were 69.3%, 27.8%, 2.9% in the case group and 62.4%, 33.0%, and 4.6% in the control group, respectively. The relative risk of ht3 +/- to -/- was 1.05 (0.55-2.01) and the relative risk of ht3+/+ to -/- was 0.60 (0.38-0.96). So, compared with the ht3 -/- genotype, the ht3+/+ genotype was significantly associated with a decreased risk of HNSCC in Koreans (P=0.03).
IL-10 polymorphisms
For the IL-10 -1082A>G SNP (genotyping was available in 628 of 648 subjects), the frequency of the variant allele G was 7% and the heterozygosity was 13.2%. The frequencies of IL-10 genotypes, -1082 AA, AG, and GG, were 85.6%, 13.7%, and 0.7% in the case group and 86.9%, 12.9%, and 0.3% in the control group, respectively. The relative risks of genotypes AG and GG to AA were 0.75 (0.40-1.43) and 1.03 (0.28-3.81), respectively. For the IL-10 +920T>G SNP (genotyping was available in 609 of 648 subjects), the frequency of the variant allele G was 30.3% and the heterozygosity was 41.2%. The genotype frequencies of TT, TG and GG were 45.5%, 46.2%, and 8.3% in the case group and 51.6%, 37.4%, and 11.0% in the control group, respectively. The relative risks of TG and GG to TT were 1.36 (0.85-2.16) and 0.88 (0.59-1.30), respectively. For the IL-10 +3917T>C SNP (genotype was available in 612 of 648 subjects), the variant allele C was 3.5% and the heterozygosity was 6.8%. The genotype frequencies of TT, TC, and CC were 92.9%, 6.8%, and 0.4% in the case group and 93.1%, 6.9%, and 0% in the control group, respectively. The relative risk of TC to TT was 0.71 (0.30-1.70). No significant statistical results were obtained in our analyses of IL-10 polymorphisms (Table 5).
IL-10 haplotypes
Two haplotypes, ht1(ATT) and ht2(AGT) for the IL-10 SNPs -1082A>G, +920T>G, and +3917T>C were analyzed. The haplotype distributions are summarized in Table 6. There was no significant difference in the distribution of the two IL-10 haplotypes in the SCCHN patient and normal control groups.
DISCUSSION
Development of cancer is dependent on individual genetic susceptibility. For example, genetic polymorphisms, activation of cancer genes and alterations of the immune system are determinants of individual genetic susceptibility (18). The most common genetic polymorphism in the population is SNP, which are single nucleotide substitutions within genes. These small changes in DNA can cause significant alterations in normal genetic function, metabolism, repair of DNA, personal sensitivity and ultimately malignant tumor development (19).
COX-2 expression and activity is induced by growth factors, carcinogens and oncogenes (20). COX-2 overexpression and its association with cancer development have been reported especially in colorectal cancer and SCCHN (21). The COX-2 gene is located at 1q25.2-q25.3 and is encoded by 10 exons (22). To date, 25 polymorphisms in the COX2 gene have been identified in a Korean sample.
Our study analyzed the association of COX-2 SNPs 1329A>G, +1266C>T, +6365T>C with SCCHN in a Korean sample. There was no definite statistical significance between cancer risk and genetic polymorphism for three COX-2 SNPs. However, the frequency of the haplotype ht3 (ACC) differed significantly. Haplotype ht3 +/+(ACC/ACC) was associated with a significantly decreased risk of SCCHN, compared with the ht3-/- group, suggesting a possible involvement of ht3 in the development of SCCHN. There has been no study that evaluates COX-2 SNPs that were analyzed in our study in SCCHN. In a study that examined the association of COX-2 -765 G>C polymorphism with the risks of oral squamous cell carcinoma in a Taiwan population, the authors reported that COX-2 -765C allele was a protective factor against oral squamous cell carcinoma (23). However, in other study in the Netherlands, there was no risk-modifying effect of COX-2 -1195 A>G and -765 G>C polymorphisms in head and neck carcinogenesis (24).
IL-10 is an important immune regulatory cytokine in humans that is mainly secreted by helper T-cells and synthesized by activated macrophages (14). The predominant effect of IL-10 is reduced inflammation, and it contributes to the control of immune-related cellular proliferation and differentiation (14, 15).
The IL-10 gene is located on chromosome 1q31-32 and is encoded in 5 exons. Numerous genetic polymorphisms in IL-10 have been reported and nearly all of them are SNPs (25). In Italian patients with undifferentiated carcinoma of the nasopharynx, it has been reported that IL-10 -1082A>G, -819C>T, and -592A>C SNPs were not associated with cancer development (26). In our study, we analyzed three IL-10 SNPs and two haplotypes. The IL-10 -1082A>G, +920T>G, and +3917T>C SNPs and their respective haplotypes were not associated with the risk of SCCHN in a Korean sample.
In conclusion, COX-2 ht3+/+ was associated with a significantly decreased risk of SCCHN in a Korean sample, compared with the COX-2 ht3 -/- genotype. Based on this result, the COX-2 haplotype ht3 can be used as a molecular biomarker to predict low risk groups of SCCHN in a Korean sample.





 XML Download
XML Download