

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
There have been many efforts for the early detection and management of diabetic nephropathy, which is the leading cause of end-stage renal disease (ESRD) (1, 2). Microalbuminuria is the initial clinical evidence and an increased albumin excretion rate (AER) is one of the most conventional parameters for the progression of diabetic nephropathy (3, 4). Measuring AER as a marker of diabetic nephropathy is based on the natural history of nephropathy in type 1 diabetes (5-10). However, in type 2 diabetes, there are many other factors that can contribute to renal insufficiency without causing albuminuria, such as atherosclerosis in renal vasculature, cholesterol emboli, and interstitial fibrosis (11, 12).
It has been reported that a decline in the renal function of patients with diabetes is not always accompanied by an increased AER (13, 14). About 20-30% of type 2 diabetics with renal insufficiency showed normoalbuminuria (12-18). In the Third National Health and Nutrition Examination Survey, the prevalence of patients with type 2 diabetes and renal insufficiency in the absence of both albuminuria and retinopathy was about 30% (12). Compared with the renal insufficiency with albuminuria, the patients with normoalbuminuric renal insufficiency were characterized by female predominance, older age, higher HDL cholesterol, lower prevalence of retinopathy, and possibly better prognosis (15-17). In addition, compared with diabetic patients with normoalbuminuria and normal renal function, patients with normoalbuminuric renal insufficiency had an increased risk of cardiovascular disease and metabolic syndrome (18-20). Therefore, normoalbuminuric renal insufficiency is a distinct entity in diabetic renal complications. However, the natural course and pathophysiologic mechanism of normoalbuminuric renal insufficiency are still elusive.
It has been shown that ESRD accounts for 10-30% of the deaths in Asian diabetic patients, which clearly contrasts with a <5-10% risk of renal death in Caucasian diabetic patients (21). Furthermore, a 4-yr follow up study showed that Asian diabetic patients are at high risk of progression to ESRD compared with Caucasian diabetic patients (22). These data suggest that Asian patients are more susceptible to diabetic renal disease compared with Caucasians. In this regard, the clinical characteristics of normoalbuminuric renal insufficiency in Asian diabetic patients might be different from their Caucasian counterparts.
We therefore performed a study on the prevalence and clinical characteristics of Korean type 2 diabetic patients with normoalbuminuric renal insufficiency and examined its relations to renin-angiotensin system (RAS) inhibitors, diabetic retinopathy, and the duration of the diabetes.
MATERIALS AND METHODS
Study population
We studied 562 randomly selected patients from the Diabetes Clinic at Seoul National University Hospital from January to December, 2006, who were diagnosed with type 2 diabetes. Excluded from this study were those patients with anti-GAD antibodies; those who started insulin therapy within the first year after diagnosis; those with a urinary tract infection, hematuria, or other causes of renal insufficiency; those with cardiac or hepatic failure; and those with a severe intercurrent illness, including malignancy. The Institutional Review Board of the Clinical Research Institute in Seoul National University Hospital approved the study protocol.
Estimation of glomerular filtration rate (GFR)
We calculated the GFR with the Modification of Diet in Renal Disease (MDRD) formula (23) and defined renal insufficiency as an estimated GFR (eGFR) of less than 60 mL/min per 1.73 m2 body surface area (BSA), which corresponded to the National Kidney Foundation Kidney Dialysis Outcomes Quality Initiative guideline (24).
Quantification of albuminuria
We measured the degree of albuminuria with spot tests of the urine albumin-creatinine ratio (ACR). Urinary albumin levels were measured by turbitimer assay (A&T 502X, A&T, Tokyo, Japan) and urine creatinine levels were measured by the Jaffe method (Hitachi 7170, Hitachi, Tokyo, Japan).
We used sex-specific ACR cut points to define micro- and macroalbuminuria (25, 26). Microalbuminuria was defined as an ACR from 17 to 250 µg/mg for males and from 25 to 355 µg/mg for females. Macroalbuminuria was defined as an ACR over 250 µg/mg and over 355 µg/mg for males and females, respectively. Albuminuria denotes the presence of micro- or macroalbuminuria.
Assessment of covariates
Questionnaires and review of the patients' medical records were used to evaluate the history of stroke, coronary artery disease, and peripheral vascular disease. Hypertension was defined as a systolic blood pressure over 140 mmHg or a diastolic blood pressure over 90 mmHg, or the fact that the patient was taking antihypertensive medications. Drug histories in relation to anti-hypertensive agents and lipid lowering agents were also evaluated. Fasting plasma glucose, HbA1c, serum creatinine, blood urea nitrogen (BUN), serum albumin, total cholesterol, triglyceride, LDL-cholesterol, and HDL-cholesterol concentrations were measured. Diabetic retinopathy was evaluated by direct fundus examination and was graded according to the modified Airlie House Classification (27).
Statistical analysis
All continuous variables with normal distributions were expressed as means±SD, while variables with skewed distributions were expressed as medians with a range. Variables not normally distributed were logarithmically transformed before statistical analysis. The results of categorical data are expressed as percentages. Student's t-test and ANOVA were used to compare the continuous variables between groups and the chi-square test was used for categorical variables. The p value for a trend was evaluated by the Mantel-Haenszel chi-square test. A level of p<0.05 was considered statistically significant. All data were analyzed using SPSS for Windows (SPSS Inc., Chicago, IL, U.S.A.).
RESULTS
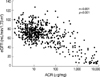
A total of 562 patients were enrolled in this study. Their mean age was 59±10 yr; the mean duration of diabetes was 8.0±7.4 yr; and their mean eGFR was 71.3±11.5 mL/min per 1.73m2. There was a significant inverse correlation between ACR and eGFR (r=-0.651, p<0.001) (Fig. 1). In the patients with eGFR <60 mL/min/1.73m2, the coefficient of correlation between ACR and eGFR slightly decreased (r=-0.552, p<0.001).
Among 562 patients, 151 (26.9%) had renal insufficiency, defined as an eGFR <60 mL/min per 1.73 m2. Among these, the prevalence of normo-, micro-, and macroalbuminuric patients was 29.1% (n=44), 33.1% (n=50), and 37.8% (n=57), respectively. After excluding the patients using RAS inhibitors (angiotensin converting enzyme inhibitors or angiotensin II receptor blockers), the number of patients with renal insufficiency was 51 and the prevalence of normo-, micro-, and macroalbuminuric renal insufficiency was 35.3% (n=18), 41.2% (n=21), and 23.5% (n=12), respectively (Table 1).
The characteristics of the 151 patients with an eGFR <60 mL/min per 1.73 m2 stratified according to their ACR, as shown in Table 2. Compared with microalbuminuric renal insufficiency, normoalbuminuric renal insufficiency was associated with female predominance, shorter duration of diabetes, lower BUN and creatinine, higher eGFR, and lower HbA1c. In addition, patients with normoalbuminuric renal insufficiency had a lower prevalence of hypertension and retinopathy, and a lower prevalence of using anti-hypertensive drugs except RAS inhibitors. Among them, female predominance, lower HbA1c, shorter duration of diabetes, lower prevalence of hypertension and retinopathy, and a lower prevalence of using antihypertensive drugs other than RAS inhibitors were still significant, even after adjusting for their eGFR. When the patients using RAS inhibitors were excluded, we obtained similar results (data not shown). Next, we compared the characteristics of the patients with normoalbuminuric renal insufficiency with those who had macroalbuminuric renal insufficiency. The results showed very similar trends to those of the comparison between normo- and microalbuminuric renal insufficiency, except for HbA1c, which was comparable between the two groups. Finally, we found that female predominance, shorter duration of diabetes, lower prevalence of hypertension and retinopathy, and a lower prevalence of using antihypertensive drugs except RAS inhibitors showed significant trends across the degree of albuminuria.
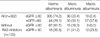
Table 3 compares the clinical characteristics of 349 patients with normoalbuminuria according to their eGFR. The patients with normoalbuminuric renal insufficiency (n=44, 12.6%) were older, more likely to be female, had a higher prevalence of using RAS inhibitors and statins, and a higher prevalence of coronary artery disease. The patients with normoalbuminuric renal insufficiency, who were not taking RAS inhibitors or statins, showed similar results but they additionally showed higher triglyceride levels (1.83 [0.59-8.20] vs. 1.69 [0.65-6.53] mM/L, p=0.03; expressed as a median [range]) and lower HDL-cholesterol levels (1.01±0.23 vs. 1.24±0.28 mM/L, p=0.02) compared to their counterparts with normal renal function.
We evaluated the trend of changes in the prevalence of normo-, micro-, and macroalbuminuric renal insufficiency along with the duration of the diabetes. The prevalence of normoalbuminuria decreased progressively, whereas the prevalence of macroalbuminuria increased with an increase in the duration of diabetes (Mantel-Haenszel χ2 test, p for trend <0.001) (Fig. 2).
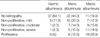
Table 4 shows the prevalence of the respective grade of retinopathy according to the AER status of the patients with renal insufficiency. The retinopathy and albuminuria were both absent in 37 of the 151 (24.5%) patients. In the normoalbuminuric renal insufficiency group, most of the patients (37 of 44 patients, 84.1%) had no retinopathy. The prevalence and severity of retinopathy were markedly and progressively increased in the micro- and macroalbuminuria groups (Mantel-Haenszel chi-square test, p for trend <0.001).
DISCUSSION
Among the Korean patients with type 2 diabetes and renal insufficiency, the prevalence of normoalbuminuria was 29.1% (35.3% in those not using RAS inhibitors). Even after adjusting for their eGFR, normoalbuminuric renal insufficiency was associated with female predominance, lower HbA1c, shorter duration of diabetes, lower prevalence of hypertension and retinopathy, and a lower prevalence of using antihypertensive drugs except RAS inhibitors compared with microalbuminuric renal insufficiency. These results are largely similar to those from Caucasian studies (15-17). The characteristics of a shorter duration of the diabetes and a lower prevalence of retinopathy found in this study suggest that normoalbuminuric renal insufficiency might be an earlier stage of renal insufficiency compared with microalbuminuric renal insufficiency. This is further supported by the results that the prevalence of normoalbuminuric renal insufficiency decreased with an increase in the duration of the diabetes and with the advanced stage of retinopathy. Thus, it might be speculated that some type 2 diabetic patients might face renal insufficiency without albuminuria and may then progress to microalbuminuric and macroalbuminuric renal insufficiency as the duration of type 2 diabetes increases. However, there are reports showing that normoalbuminuric renal insufficiency was not associated with a lower prevalence of retinopathy (15, 16). Furthermore, Rigalleau et al. (17) reported that diabetic patients with normoalbuminuric renal insufficiency showed stable AER over 38 months and had a low risk for the progression to ESRD or death. Therefore, to support our hypothesis that normoalbuminuric renal insufficiency might be an earlier stage of diabetic renal complication, we need a prospective study including looking into the change of renal pathology.
In the next step, we examined whether there was any difference in the clinical characteristics of normoalbuminuric patients according to their eGFR. Compared with the patients with normoalbuminuria in the absence of renal insufficiency, those with normoalbuminuric renal insufficiency were older, more likely to be female, had a higher prevalence of using RAS inhibitors and statins, and a higher prevalence of coronary artery disease. The higher prevalence of coronary artery disease suggests that other atherosclerotic diseases involving the renal vasculature might be responsible for the decreased renal function in the absence of albuminuria. In this regard, a recent report (18) also showed that normoalbuminuric renal insufficiency was associated with metabolic syndrome. However, MacIsaac et al. (16) found that patients with type 2 diabetes and reduced GFR had similar degrees of intrarenal vascular disease, assessed by the intrarenal arterial resistance index. Therefore, at this time, the mechanism of normoalbuminuric renal insufficiency still remains elusive. Interestingly, genetic susceptibility might play a role in the development of normoalbuminuric renal insufficiency. It has been reported that polymorphisms of the protein kinase C-β gene (PRKCB1) were associated with diabetic nephropathy that did not lead to albuminuria in Japanese patients (28).
A female predilection for normoalbuminuric renal insufficiency has been noted in many other previous studies (14, 15, 17, 18), but the reason for this association is unknown. In this study, the patients with normoalbuminuric renal insufficiency were more likely to be females over 50 (odds ratio [OR] and 95% confidence interval [CI] was 3.08 [1.15-4.13], p=0.017), while we could not find this age effect in male subjects (OR and 95% CI was 1.38 [0.48-3.26], p=0.646) (data not shown in the Results). Therefore, the pathogenesis of normoalbuminuric renal insufficiency might be affected by the hormonal change that occurs around menopause.
There were several limitations in this study. First, owing to the cross-sectional design it was difficult to clarify the causal relationship between the risk factors and the natural course of the normoalbuminuric renal insufficiency. Second, the eGFR might not reflect the actual GFR of our study population, since the MDRD study included very few Asians (29). Third, the assessment of AER with a single specimen might not exactly estimate the number of normoalbuminuric renal insufficiency. Finally, the number of the patients with renal insufficiency not taking RAS inhibitors was somewhat small. Therefore, a further study including sufficient number of patients in this category is necessary.
In conclusion, normoalbuminuric renal insufficiency was prevalent in type 2 diabetic Korean patients and the clinical characteristics were largely similar to those seen in previous studies. The association with a shorter duration of the diabetes and a lower prevalence of retinopathy suggests that normoalbuminuric renal insufficiency might be an early stage renal complication in Korean type 2 diabetic patients.



 XML Download
XML Download