

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Early detection and correction of the risk factors for diabetic nephropathy (DN) might slow the development or progression of DN. The urinary albumin excretion rate (AER) is the mainstay in early detection of DN (1). In addition, several factors such as hypertension, hyperglycemia, genetic predisposition, retinopathy, age, dyslipidemia, family history, smoking history, and the amount and origin of dietary protein were also suggested as predictors of DN risk in individual patients (1, 2).
Cardiac autonomic neuropathy is an early and common complication of diabetes mellitus (DM) (3). Previous studies have reported that cardiac autonomic neuropathy might be a risk factor for DN and associated with deterioration of renal function in people with DM (4-16). However, there are not enough longitudinal data to show that cardiac autonomic neuropathy could be an early predictor of deterioration of renal function in normoalbuminuric, normotensive diabetics, especially in patients with type 2 DM. The aim of our study, which was performed retrospectively, was to evaluate whether cardiac autonomic neuropathy, as an early complication of DM, is associated with deterioration in glomerular filtration rate (GFR) in normoalbuminuric, normotensive patients with type 2 DM.
MATERIALS AND METHODS
Patients
This retrospective longitudinal study was performed in accordance with the principles of the 1983 Declaration of Helsinki. From January 1996 to June 1997, consecutive patients with type 2 DM, who had undertaken the cardiac autonomic function test as one of the initial screening tests of diabetic complications at the Samsung Medical Center, Seoul, Republic of Korea, were eligible for inclusion if they 1) had systolic blood pressure of less than 130 mmHg and diastolic blood pressure of less than 85 mmHg; 2) had a urinary AER of less than 20 µg/min; 3) had an initial serum creatinine level noted at the time of the cardiac autonomic function test and a follow-up serum creatinine level recorded at least 9 yr from that time; 4) had no evidence of cardiac or renal disease at the time of the cardiac autonomic function test; and 5) had no history of antihypertensive medication at the time of the autonomic function test. Type 2 DM was diagnosed if they 1) had no episodes of ketoacidosis; 2) diagnosed DM after the age of 40 yr; 3) treated by diet alone, or in combination with oral hypoglycemic agents or fasting serum C-peptide values greater than 1.0 ng/mL in patients administered with insulin.
When multiple follow-up creatinine levels were available, we used the most recent value, and excluded values that were associated with an acute illness or hospitalization. One hundred and 56 patients met the inclusion criteria.
Cardiac autonomic function tests
We conducted five tests for each patient to evaluate cardiac autonomic function. Three tests to assess parasympathetic neuropathy were heart-rate response to deep breathing, standing up and the Valsalva manoeuvre. Two tests to assess sympathetic neuropathy were blood-pressure response to sustained handgrip and standing up. The methods of each test are described below (17).
Heart-rate response to deep breathing
Six maximal expirations and inspirations were performed within one minute in the supine position, during which heart rate was continuously recorded by electrocardiography (ECG), and the R-R intervals were recorded. The E/I ratio was calculated as the mean of the longest R-R interval during expiration (E) divided by the mean of the shortest R-R interval during inspiration (I). 'Abnormal' was defined as a ratio of less than 1.00; 'borderline' as a ratio of 1.01-1.09; and 'normal' as a ratio of more than 1.11.
Heart-rate response to standing up
The patient lay quietly and stood up unaided. The heart rate was recorded continuously by ECG. The '30:15 ratio', which is the ratio of the longest R-R interval (around the 30th beat after starting to stand up) to the shortest R-R interval (around the 15th beat), was then calculated. 'Abnormal' was defined as a ratio of less than 1.00; 'borderline' as a ratio of 1.01-1.03; and 'normal' as a ratio of more than 1.04.
Heart-rate response to the Valsalva manoeuvre
The patient sat quietly and then blew into a mouthpiece at a pressure of 40 mmHg for 15 sec. Heart rate was recorded continuously using ECG during and after the manoeuvre. The ratio of the longest R-R interval shortly after the manoeuvre to the shortest R-R interval during the manoeuvre was then calculated. 'Abnormal' was defined as a ratio of less than 1.10; 'borderline' as a ratio of 1.11-1.20; and 'normal' as a ratio of more than 1.21.
Blood-pressure response to sustained handgrip
The patient squeezed a handgrip dynamometer as hard as possible for a few seconds and then maintained steady pressure at 30% of the maximum pressure for three to four minutes. Blood pressure was measured each minute, and the difference between the diastolic blood pressure before starting and that just before the release of the handgrip was measured. 'Abnormal' was defined as a difference of less than 10 mmHg; 'borderline' as a difference of 11-15 mmHg; and 'normal' as a difference of more than 16 mmHg.
Blood-pressure response to standing up
Blood pressure was measured while the patient was lying down and again one minute after standing up, and the difference in systolic blood pressure was noted. 'Abnormal' was defined as a difference of more than 30 mmHg; 'borderline' as a difference of 11-29 mmHg; and 'normal' as a difference of less than 10 mmHg.
Classification of test result
We categorized the results of these five tests as: 'normal pattern', all tests normal or one borderline; 'early pattern', one of the three heart-rate tests abnormal or two borderline; 'definite or severe pattern', two or more of the three heart-rate tests abnormal (definite pattern), or definite pattern plus one or both of the blood-pressure results abnormal, or both borderline (severe pattern); 'atypical pattern', any other combination of abnormal tests.
Clinical information and laboratory data
Clinical information was assessed from written and electronic medical records, which included medical history, current medications and laboratory data. The data collected included age, sex, urinary AER, serum creatinine, systolic blood pressure, diastolic blood pressure, retinopathy, glycosylated hemoglobin level (HbA1c), total cholesterol level, high-density lipoprotein (HDL) cholesterol level, low-density lipoprotein (LDL) cholesterol level, triglycerides level, homeostasis model for insulin resistance (HOMA-IR), body fat mass (%), use of statin, use of aspirin, duration of diabetes and estimated GFR. Urinary AER was assessed on 24 hr urine collection. Normoalbuminuria was defined as less than 20 µg/min in 2 out of 3 consecutive tests taken within 2-3 months. Blood pressure was measured twice, 5 min apart, using a random zero sphygmomanometer with the patient seated after 10 min of rest. Based upon the average of readings at each of two or more visits, hypertension was defined as a systolic blood pressure of more than 140 mmHg and/or a diastolic blood pressure of more than 90 mmHg for three months and/or the commencement of antihypertensive therapy. The presence of retinopathy was assessed by fundus photography, which was interpreted by ophthalmologist. HOMA-IR (%), index of insulin resistance, was calculated by the formula, fasting glucose/18×insulin/22.5, with insulin expressed in µU/mL and fasting glucose in mg/dL (18). Body fat mass (%) was measured in a bioimpedance analysis (Inbody 2.0, Biospace, Seoul, Korea). Estimated GFR was calculated using the Modification of Diet in Renal Disease four-variable equation at the time of the cardiac autonomic function test (19). During the follow-up period, we also calculated estimated glomerular filtration rate (eGFR) using the chemistry profile at the last visit.
Statistical analysis
Demographic, clinical, and biochemical data are expressed as means±SD. We used a paired t test to compare differences in continuous variables within the groups. One-way ANOVA test or Kruskal-Wallis test was used to compare differences in continuous variables, and the chi-square test or Fisher's exact test to compare categorical variables among groups. The association of the change of eGFR with demographic, clinical or biochemical variables were determined using univariate linear regression analysis. Multivariate linear regression analyses were conducted to detect independent predictors of eGFR decline. Kaplan-Meier life-table analysis was used to calculate the cumulative incidence of hypertension during follow-up period. A p value of <0.05 was considered statistically significant. All statistical analyses were performed with SPSS 12.0 for Windows (SPSS, Chicago, IL, U.S.A.).
RESULTS
Of 156 patients, 54 had normal patterns on the autonomic function test, 75 had early patterns, 25 had definite or severe patterns, and 2 had atypical patterns. The prevalence of cardiac autonomic neuropathy was 65.4% in normoalbuminuric, normotensive stage. Forty-one patients had concordant abnormal heart-rate response to deep breathing, 59 concordant abnormal heart-rate response to standing up, 29 concordant abnormal heart-rate response to the Valsalva manoeuvre, 6 concordant abnormal blood-pressure response to sustained handgrip and no patient concordant abnormal blood-pressure response to standing up. Two patients with atypical patterns were eliminated from the analysis because their number was too small to obtain statistically valid results. The characteristics of the patients, based on their patterns of autonomic function are given in Table 1. There were no significant differences in sex, serum creatinine, eGFR, urinary AER, systolic and diastolic blood pressure, HbA1c, retinopathy, lipid profiles and body fat mass at baseline among the three groups. There were also no significant differences in numbers of patients with treatment with statin and aspirin among the groups. However, the definite or severe pattern group was older and had DM longer than the other groups. HOMA-IR values in the early pattern group were significantly higher than those in the normal pattern group.
Median follow-up duration was 9 yr. During the follow-up period, there was no significant difference between the baseline eGFR and the last follow-up eGFR in the normal pattern and early pattern groups. However, in the definite or severe pattern group, eGFR decreased significantly. In an intergroup comparison, the definite or severe pattern group had a greater change in eGFR than that of the normal pattern group or early pattern group (Table 2).
Predictors of a decline in renal function
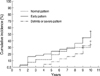
Table 3 shows the univariate analyses for relationship of the change of eGFR with clinical parameters at baseline of the study. The decline in eGFR was associated with an abnormal heart-rate response to the deep breathing test, age, eGFR, total serum cholesterol level and diabetic retinopathy. Sixty-two patients progressed to hypertension during the follow-up period. Seventeen of the 54 patients with normal pattern of cardiac autonomic neuropathy progressed to hypertension, as did 36 of the 75 patients who had an early pattern and 9 of the 25 patients who had a definite or severe pattern. There was no significant difference in the incidence of the development of hypertension among the different patterns of cardiac autonomic neuropathy (Fig. 1). However, new-onset hypertension during the follow-up period was associated with the decline in eGFR (Table 3, 4). Multivariate linear regression analysis was conducted to determine the independent predictors affecting the decline of eGFR. The heart-rate response to the deep breathing test, age, diabetic retinopathy and new-onset hypertension during follow-up period were independently and significantly related to the decline in eGFR (Table 4).
DISCUSSION
Previous studies have demonstrated a significant relationship between cardiac autonomic neuropathy and decline in GFR in individuals with DM (4-12). Previous studies also showed that cardiac autonomic neuropathy is one of the early complications of DM and exists even at the normoalbuminuric, normotensive stage (3, 4). There are few longitudinal data that demonstrate whether cardiac autonomic neuropathy has a close relationship to the deterioration of renal function in the normoalbuminuric, normotensive stage. In our study, we enrolled 156 subjects with type 2 DM with normoalbuminuria and normotension at the baseline and followed up for about 9 yr retrospectively. The results showed that the prevalence of cardiac autonomic neuropathy was 65.4% and cardiac autonomic neuropathy was one of the significant predictors of decline in renal function in normotensive, normoalbuminuric subjects.
The underlying mechanism by which cardiac autonomic neuropathy may lead to nephropathy is reported in previous studies (11-16). If sympathetic neuropathy is dominant, renal sodium excretion and renal blood flow are diminished, and the GFR is decreased via vasoconstriction in the kidney. If parasympathetic neuropathy is dominant, systolic hypertension, resting tachycardia, and increased cardiac output develop, which injure the glomerular membrane, causing an increase in albumin leakage through the glomerular membrane. Our study showed that parasympathetic neuropathy (i.e., abnormal heart-rate response to the deep breathing test) affected GFR whereas sympathetic neuropathy did not. This finding may be related to the small number of patients with sympathetic neuropathy in our study, which showed the low prevalence (3.9%) of sympathetic neuropathy in the normoalbuminuric, normotensive stage. A large number of subjects with sympathetic neuropathy or 24-hr ambulatory blood pressure monitoring-instead of blood pressure response to sustained handgrip and blood-pressure response to standing up-will clarify the relationship of sympathetic neuropathy with a deterioration of renal function (14-16).
In our study, in addition to abnormal heart-rate response to the deep breathing test, age and diabetic retinopathy were also independent and significant risk factors for a decline in GFR. These findings are similar with previous study, which reported that baseline plasma creatinine, systolic blood pressure, age at diagnosis, height, Indian-Asian ethnicity, ever smoking, previous retinopathy, and urinary albumin were independently associated with increased risk of development of reduced creatinine clearance in patient with type 2 DM (20).
The baseline levels of HbA1c were relatively high among three groups in our study because patients with naive type 2 DM and high blood glucose level were also enrolled. But the levels of HbA1c were not associated with a deterioration of renal function and decreased equally with treatment during the follow-up period.
The cumulative incidence of development of hypertension was 37% during the follow-up period. Previous study reported that Cardiac autonomic neuropathy is independently associated with hypertension in normoalbuminuric Type 2 diabetic patients with no history of hypertension (21). In our study, there was no significant difference in the incidence of the development of hypertension among the different patterns of cardiac autonomic neuropathy. Larger prospective study will clarify the relationships between cardiac autonomic neuropathy and hypertension in patients with type 2 DM. In our study, although there was no significant difference in microalbuminuria between the patients with new-onset hypertension and without new-onset hypertension (7.0±5.0 µg/min vs. 6.0±4.3 µg/min, p=0.180), eGFR decreased significantly in patients with new-onset hypertension compared with the patients without new-onset hypertension (% eGFR change from baseline, -8.0±27.5 vs. 5.9±17.2, p=0.001). New-onset hypertension during the follow-up period was an independent and significant risk factor for a decline in GFR.
In our study, 53 of the 62 patients with hypertension during the follow-up period were treated with angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB). The use of ACEI or ARB was not associated with change of eGFR, which is different from previous studies (22, 23). Twenty-six of 53 patients prescribed ACEI or ARB took more than two anti-hypertensive agents and all of 9 patients who were not prescribed ACEI or ARB took only one anti-hypertensive agent that may be why the use of ACEI or ARB did not conferred significant renal benefit in our study.
Previous data reported that diabetic parasympathetic neuropathy affects the insulin resistance in type 2 diabetic patients (24). In our study, HOMA-IR, an index of insulin resistance, was higher in group with an early pattern than in the group with a normal pattern. However, HOMA-IR had no significant relationship with eGFR decline.
The results of our study revealed that cardiac autonomic neuropathy was an important predictor of decline in GFR, however, risk factors that were not analyzed in our study should be also considered. Development of microalbuminuria or control of hyperglycemia during follow-up period may affect decline in GFR. We could not exclude the potential role of these factors in deterioration of renal function during follow-up period. And our study was performed retrospectively so there were quite heterogeneous patients among three groups, in particular in terms of duration of diabetes and patient's age, which was one of the limitations of our study. Therefore, we cautiously conclude that cardiac autonomic neuropathy may be considered as one of the risk factors in deterioration of the renal function in normoalbuminuric, normotensive patients with type 2 diabetes mellitus.
In conclusion, cardiac autonomic neuropathy could be present at the normoalbuminuric, normotensive stage. Cardiac autonomic dysfunction could be associated with deterioration of GFR in normoalbuminuric, normotensive patients with type 2 DM and may be an early predictor of DN.




 XML Download
XML Download