

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Systematic and effective welfare for the disabled requires scientific and objective criteria demonstrating either presence or severity of the impairment accurately (1, 2). However, there has been distrust and dissatisfaction since current criteria measuring disability or physical impairment have brought significant diagnostic errors, fakers, or malingers (2-7). The criteria or definition of the physical impairment differ from country to country (8, 9). Since the disability is influenced by culture and society, we need our own scientific criteria suitable for Koreans. Currently, we have about 30 methods or criteria measuring the degree of disability including those under the Industrial Accident Compensation Insurance Act and the Korean Welfare of Disabled Persons Act. Even though the disability is the same, the degree of disability differs according to the measurement criteria or methods. Not only does the difference itself cause confusion, but also every citizen has to visit the hospital to get the suitable disability certificates. In the U.S.A., they have their own scientific and systematic guidelines for the evaluation of permanent physical impairment (American Medical Association [AMA] Guides, 5th ed) (10). We need our own scientific guidelines suitable to our culture and society. The purpose of this project is to develop a scientific and objective method for disability evaluation suitable to Korean culture and society.
MATERIALS AND METHODS
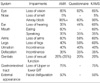
Under the supervision of Korean Academy of Medical Sciences (KAMS), we organized 13 committees with medical specialists who had experiences and knowledge of disability medicine (Fig. 1).
We studied the backgrounds and purpose of the guidelines for disability evaluation, basic concepts and principles of disability evaluation. We examined and compared several guidelines including the AMA guides, Euroguideline, McBride's method (11), California's Permanent Disability Rating Schedule (12), and so on. By modifying the most suitable methods from those guides, we developed a new KAMS Guideline for Impairment Evaluation (KAMS Guideline) compatible to Korean way of thinking and culture.
We developed the KAMS Guideline according to the following basic principles. The KAMS Guideline should be scientific, objective, valid, reasonable and practical. Objectivity was the most important value.
Impairment evaluation should be done when the symptoms are fixed. The impairment should be re-evaluated every 2 yr, when we expect any changes in symptoms, even though the symptoms are stable at present.
Medically measurable impairment should be fixed, rigid, un-recovered symptoms after a thorough medical treatment. Causes of the impairment may not be trauma. The impairment may come from congenital disorders or diseases. The impairment should be evaluated by medical specialists who are expert in their fields.
We proposed the maximum whole person impairment rating of a certain organ or a part of body system according to the following principles.
1) It was 100% whole person impairment rating when total loss of function of a given organ may cause death, such as liver, lung, heart, and so on. The degree of whole person impairment was rated by a relative degree of impairment or dysfunctions of a given organ.
2) When total loss of any function of a given organ could not cause death, such as eyes, nose, ears, mouth, arms, legs, and so on, the degree of whole person impairment was rated by two references, i.e., AMA Guides and the Korean consensus (13).
When there are multiple impairments, we can adjust them by the following manner. Body systems in impairment evaluation were classified into 11 systems (Fig. 1) instead of 8 systems of the International Classification of Functioning, Disability and Health (ICF) frame (14, 15). When the impairments were in the same organ or body system, we rated the most severe impairment only. When the impairments occurred in different organs or body systems, the final degree of physical impairment was the combination of the impairments. If a minor impairment occurs independently and it is not a subset of the major impairment, the impairments can be combined. If the minor impairment always accompanies with the major impairment, we rated the most severe impairment only.
RESULTS
In March 2007, we had a workshop on the basic concepts and knowledge on the disability evaluation and welfare system for the disabled. We invited more than 100 board certified specialists from 15 medical societies for this study. We organized 13 committees with the medical specialists. In each committee, they prepared a basic frame for the disability evaluation through monthly intrinsic meetings.
In May 2007, we had an international symposium on the disability evaluation. We invited three foreign speakers from Australia, Japan, and U.S.A. They gave us some important aspects of the disability evaluation system. We also presented the basic frame of the KAMS Guideline at the symposium in detail and discussed the subjectivity, validity, and weak points of the guideline.
We proposed the maximum whole person impairment rating of a certain organ or a part of body system. The Korean consensus on the impairment was reported in 2006 (13). A questionnaire survey was conducted on the severity of the two different physical impairments in the Korean public. They thought that the vegetative state was a severe impairment than quadriplegia. Paraplegia was regarded as severe than loss of the legs. Loss of one arm was considered severe than lumbar multi-segment fusion. They also thought that loss of one leg, hearing loss, mental retardation, and loss of one arm were almost the same degree of impairment (Table 1).
A questionnaire survey was also conducted by Korean doctors on the severity of different physical impairments. The degree of impairment was severe in quadriplegia than in total blindness. Loss of vision was regarded as a severe impairment than paraplegia (Table 2).
Although the Korean public thought that loss of the legs was severe than loss of the arms (40.9:26.0), the Korean doctors answered that the loss of arms was severe than loss of the legs (24.2:55.9).
By the results of questionnaires and AMA Guides, we decided the maximal degree of whole person impairment in a certain organ or a part of body by the following steps. If the rate of AMA Guides was similar to the result of the questionnaire survey, we accepted the rate of AMA Guides. If the rate of AMA Guides differed from the result of the survey, the degree was modified after a discussion at the steering committee. For example, the committee decided the relative importance of the arms and legs 50:50. There were not enough reasons to change the existing standards now, since the public consensus differed from the doctors' opinions. If there were significant differences between the Korean consensus and the AMA Guides, the degree of impairment was determined after thorough discussion within the steering committee. Although the loss of vision was 100% loss of work ability in the Industrial Accident Compensation Insurance Act, the rate of physical impairment was 85%, the same as the AMA Guides. The hearing loss was rated as 60%, higher than the rate of the AMA Guides (35%), lower than the rate of the Industrial Accident Compensation Insurance Act (Grade 4, 90%) (Table 3).
We had several business meetings with the government. The Korean Welfare of Disabled Persons Act approved only 15 types of disabilities, grading them into 6 steps. The basic frame of the KAMS Guideline differed from the present the Korean Welfare of Disabled Persons Act. There is a need to develop a new system; however, sudden change of the disability evaluation system may cause a great confusion. Besides the subjectivity and validity of the guidelines, it is a big dilemma making a new system without destroying the present grading system.
Finally we reported the KAMS Guideline for the 15 types of disabilities with an appendix including the remaining types of disabilities.
DISCUSSION
The guidelines for impairment evaluation are a sum of science and consensus (12). The KAMS Guidelines are medically evaluating guidelines for physical impairment, the same as the AMA Guides. To be scientific, we benchmarked the AMA Guides. The AMA Guides are scientific with public trust, which can be used as a global standard (4). To get objectivity, we avoided a decision based on subjective symptoms. We actively developed some scoring methods, summation of several scores representing the degree of objective signs or results of many different tests. To be valid, we introduced a comprehensive measurement representing the whole function instead of focal details. To be reasonable, we made the sum of different impairments of the body region which was never larger than a loss of the body region. We also reflected the results of the questionnaire survey. The degree of physical impairment is influenced by the society and culture (2, 8, 9). Criteria of impairment or non-impairment may be different depending on the society and culture. The degree and status of the impairment can be changed by the environment, too. The concept and criteria assessing the degree of physical impairment differ from country to country. To be practical, we considered the public transport system for the disabled in Korea. We also considered medical environment of Korea, since we cannot objectively measure all impairments by rarely deployed expensive equipments.
We measured medically assessable physical impairments, although the kinds and criteria of the physical impairment may vary greatly. We did not include impairments from dental problems. We also excluded some physical impairment, which originated from the concept of herbal or oriental medicine. The medically assessable physical impairments should be fixed permanently, but not temporarily. The term permanent means that the impairment is not expected to change by more than 3% over the ensuing year for the whole body impairment rating (12).
We could not confirm the whole person impairment rates, when the experts could not come to an agreement. We left them till an agreement is possible by a new method or criteria.
To objectively demonstrate the physical impairment, we should confirm any objective evidences by current medical diagnostic methods. Objective evidences include not only structural or anatomical abnormalities, but also functional disturbances. Medically demonstrated evidences may include an agreement of at least 70% of the experts. For the controversial kinds of impairment, a special committee may discuss and decide them.
Since the cardiopulmonary functions are usually dynamic, symptoms and the degree of impairment of these functions may depend on the treatment. In this situation, it is very difficult to differentiate disorders from the impairment. Anyway, the degree of impairment may be increased by improper treatment, which may promote voluntary improper treatment for higher degree of impairment. In the KAMS Guideline, we tried to induce proper treatment by making the history of medical treatment as one of the scoring components. We tried to avoid faking by scoring methods, summation of several scores representing the degree of objective signs or results of many different tests. Assurance of the objectivity by scoring methods and promotion of the proper treatment can be distinctive methods. We reserved impairment rating on the pain untill a valid measurement is developed, since the pain cannot be assessed objectively yet (16, 17).
Body systems in impairment evaluation can be important to adjust the degree of impairments when there were multiple different physical impairments. Those can be used to decide whether or not, or extent of welfare service according to the impairment pattern, rate or body systems. In the Industrial Accident Compensation Insurance Act, the whole person is classified into 10 regions (eye, ear, nose, mouth, head and neck, mental and nervous system, chest and abdomen, body column, arms, and legs), which is further divided into 25 body systems according to whether the impairment is structural or functional. McBride's method classified the whole person into 14 body systems, while the AMA Guides divided it into 15 body systems. The Korean Welfare of Disabled Persons Act divided into physical impairment and mental impairment. Physical impairment was further divided into internal and external, and finally into 15 subclasses. In ICF of WHO, impairment due to body function or structure was listed in 8 chapters (15). In the future, many countries are expected to use the ICF classification system. However, the ICF system is not yet practical. In the KAMS Guideline, body systems were classified 11 systems instead of the ICF chapters.
Although we proposed the maximum whole person impairment rating of a certain organ or a part of body system, the final rate of the maximum whole person impairment will be determined by another survey, which will be done on the next year.
The concept and criteria measuring disability or physical impairment may depend on the purpose. In general, medically evaluated physical impairments represent the degree of difficulty in usual activities of daily living except job or work. The KAMS Guideline is for assessment of the physical impairment; in other words, a medical impairment. The medical impairment can be measured objectively and scientifically by doctors. It can be used for a reward of impairment when we do not need to consider occupation or workability.
The rate of labor loss represents a competence of a certain occupation or workability; in other words, an economical impairment. The rate of labor loss can be calculated by multiplying the medical impairment by a labor coefficient. The labor coefficient may be developed often considering the difficulty or importance of a certain job or a task and the function of a certain organ or part of body. The rate of labor loss can be used for a compensation or reparation of the economic loss by the physical impairment.
For proper welfare for the disabled, we need other kinds of impairment representing the individual variable demands in addition to the medical impairment, which usually lacks individual socioeconomic and environmental factors. The welfare impairment can be calculated by multiplying the medical impairment by a welfare coefficient. The welfare coefficient may be developed often considering the need of self-care, education or rehabilitation.
Study provided that regulations of the 23 acts related to impairment assessment and analyzed according to the authorities in charge (Table 4). There were a total of eleven authorities in charge by 2005: nine departments, one office and one committee. The many authorities and acts that apply different impairment assessment standards and levels give rise to a variety of subjects. In addition, the disabled experience inconvenience and loss in expenses because they have to have different impairment diagnoses for the same impairment. Furthermore, there are also problems such as fraudulent acquisition and illegal supply and demand of impairment levels that utilize the complex process conversely. In particular, analysis of impairment levels according to organs of the body in 15 acts led to the conclusion that there are diverse structures of levels by each act for the impairment condition of the same organ and that there is a lack of consistency. In addition, only three acts- the Industrial Accident Compensation Insurance Act, the Act on Honorable Treatment and Support for Persons of Merits of National Contribution, and the Government Employee Pension Act-present methods of determining impairment levels; the other acts provide vague standards of disability levels, using terms such as "obvious" and "definite". Those who determine the impairment levels are left to use their personal standards to make decisions and as a result, there is also a lack of objectivity and rationality in the determination of impairment levels (18).
Similar to these variable coefficients, we can get many different kinds of impairments suitable for the purpose of variable acts. To develop these variable coefficients, cooperative investigation of the medical and other fields is necessary.
In conclusion, we develop the KAMS Guideline for Impairment Rating, which is most appropriate for Korean consensus, social systems and medical environment, by modifying the AMA Guides.




 XML Download
XML Download