

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
CD4+CD25+ T regulatory cells (Tregs) with the ability to suppress the function of normal responder T cells were first described by Sakaguchi et al. (1). Tregs are typically hyporesponsive to antigenic stimulation and able to suppress the proliferation and activation of both CD4+ and CD8+ T cells, thus resulting in allograft tolerance (2, 3). These suppressive mechanisms include stimulation through the T-cell receptor by specific antigen, direct cell to cell contact, signaling by cytokines, such as Interleukin (IL)-10, IL-4 and transforming growth factor-β, and signals via costimulatory molecules such as CTLA-4, CD28 and glucocorticoid-induced TNF receptor (4, 5). Studies in rodents have shown that Tregs can also play a central role in allograft rejection in transplantation (6).
After transplantation, Tregs are usually found in recipient lymphoid tissue and at the graft site (7, 8). Tregs in both sites can block the initiation of an immune response against the graft. Tregs, which represent approximately 5-10% of peripheral circulating CD4+ T cells in rodents and humans, have also been isolated from the peripheral blood of recipients (9); however, there is little information about the clinical significance of circulating Tregs in kidney transplantation. This study aimed to evaluate the clinical significance of circulating Tregs in transplantation during the early posttransplant period when the immunologic response between host and graft is active and strong immunosuppression is needed to prevent acute rejection. In our study, we evaluated the association between the frequency of circulating Tregs and clinical parameters that may affect the level of Tregs. The results of our study suggest that the frequency of circulating Tregs is associated with types of immunosuppressants and rejection process during the early posttransplant period.
METERIALS AND METHODS
Study population and control
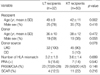
Total of 50 consecutive kidney transplant (KT) recipients were studied. As controls, 32 liver transplant (LT) recipients and 29 healthy controls (HC, 19 males, mean age 44±13 yr) were included. All transplant recipients received an allograft at the Kangnam St. Mary's Hospital between January 2006 and January 2007. The clinical characteristics are shown in Table 1. There were no significant differences among groups except for recipient age. In KT recipients, the renal function of the patients was excellent (serum creatinine 1.2±0.3 mg/dL) at the time of protocol biopsy (n=42), however, the subclinical AR (SCAR) showed in the 11 (26%) of 42 patients. And one patient died with a functional graft 3 month after transplantation because of cytomegalovirus infection.
Study design
After receiving informed consents, peripheral blood samples were obtained in HC, KT and LT recipients. In kidney transplantation, blood sample was withdrawn before transplantation and 1, 2, and 8 weeks after transplantation. In liver transplantation, blood sample was obtained before transplantation and 1 and 2 weeks after transplantation. After transplantation, peripheral blood was consequently drawn before intake of immunosuppressant. Protocol biopsy was performed at 14 days post transplant.
Immunosuppressive regimens
All patients received intravenous methylprednisolone (1 g per day) on the day of transplantation, and then oral prednisolone was tapered down to 30 mg/day on the fourth day of transplantation. We divided the KT patients into 3 groups according to the immunosuppression: FK group (n=28) (Basiliximab+Prednisolone+FK506+MMF), CsA groups (n=12) (Basiliximab+Prednisolone+CsA+MMF) and CsA/mTORi groups (n=10) (Prednisolone+CsA+sirolimus/everolimus). Initial CsA dose was 10 mg/kg per day by oral route, and target trough levels were 200-400 ng/mL in the first 4 weeks and 100-200 ng/mL thereafter in the CsA based immunosuppresion, 100-200 ng/mL in the first 4 weeks and 75-150 ng/mL thereafter in the CsA/everolimus group. Initial FK506 dose was 0.16 mg/kg per day by oral route, and target trough levels were 10-15 ng/mL in the first 3 months. Initial dose of MMF was 1.5 g/day, and dose was modified based on adverse effects such as diarrhea or leucopenia. IL-2 receptor blocking antibody (anti-IL-2R Ab, Basiliximab) was given to 40 patients (CsA or FK506 based immunesuppression) 4 hrs before and 3 days after renal transplantation. Everolimus was administered 1.5 mg per day and sirolimus was loaded 6 mg per day and then adjusted dose of 2 mg/day was maintained with target trough level of 5-15 ng/mL. In LT recipients, mycophenolate mofetil, cyclosporine, and prednisolone were given as standard immunosuppression.
Clinical parameters
The potential factors which may affect circulating Tregs were included. The type of underlying disease of end stage renal disease (ESRD), the number of HLA mismatch, panel reactive antibody (PRA), the age and sex of donor and recipients, subclinical acute rejection (AR), episode of BK virus (BKV) and cytomegalovirus (CMV) infection), graft function and cyclosporine/FK506 serum concentrations were evaluated.
The diagnosis of CMV infection was made when copy number of by real time polymerase chain reaction (RT-PCR) is more than 2,000 copies/mL or with tissue biopsy, and the diagnosis of BKV infection was made when copy number of RT-PCR is more than 10,000/mL in peripheral blood. Subclinical rejection was defined as either borderline/suspicious or acute subclinical rejection in patients with stable serum creatinine values at the time of biopsy (10). A test for the panel reactive antibody (PRA) was performed by ELISA PRA (LATM, One-Lambda Inc, CA, U.S.A.). More than 20% of PRA was regarded as positive PRA. Delayed graft function (DGF) was defined as the need for dialysis during the first week after transplantation. Graft failure was defined as returning to dialysis.
Flow cytometric analysis
Peripheral blood lymphocytes were stained with CD4-FITC (Dinona, Seoul, Korea) and CD25-PE-Cy7 (BD Pharmingen, San Diego, CA, U.S.A.). The percentages of CD4+CD25+ cells were analyzed using a Coulter EPICS XL (Beckman Coulter, Miami, FL, U.S.A.). Lymphocytes were gated on the basis of light scatter characteristics and at least 10,000 events were obtained for each patient sample. The lymphocyte purity of ≥98% of gated populations was confirmed with staining of a CD45-FITC antibody (Dinona).
ELISPOT assays
The Interleukin-10 ELISPOT assay was performed using a commercial kit (eBioscience Co, San Diego, CA, U.S.A.) as previously reported (11). Peripheral blood lymphocytes (PBLs) were freshly isolated by Ficoll density gradient. PBLs from the recipients (200,000 cells/well) in 100 µL of culture medium were placed in 96-well ELISPOT plates that were precoated with capture anti-IL-10 antibody, and PBLs (200,000 cells/well) from donor lymphocytes. Stimulator cells were used after 3000 rad (30 Gy) irradiation, and all assays were performed under sterile conditions. Plates were then incubated overnight at 37℃. Following three washes with washing buffer, a biotinylated detection antibody was added to the wells (100 µL/well), and the plates were incubated for 2 hr. After an additional wash, anti-streptavidin horseradish peroxidase was added for 45 min at room temperature. After a final wash, the plates were developed with aminoethylcarbazole (10 mg/mL in N,N-dimethylformamide; Pierce Chemiclas, Rockford, IL, U.S.A.), prepared in 0.1 M sodium acetate buffer (pH 5.0) mixed with H2O2. The resulting spots were counted with AID ELISPOT analyzer (Autoimmun Diagnostika, Germany).
Statistical analysis
The data were expressed as mean±SD or median and interquartile ranges (IQR) (25-75th percentiles). For continuous variables, statistical significance was assessed by Student's t-test or, if the variable deviated from a normal distribution, by nonparametric tests (Mann-Whitney). The statistics were performed with Windows SPSS 10.5. A two-tailed p value of <0.05 was considered to be statistically significant.
RESULTS
The frequency of Tregs before transplantation
Fig. 1A shows the comparison of the frequency of Tregs before transplantation in KT and LT recipients and in healthy controls. The median frequencies of Tregs in KT recipients and healthy controls were 4.2% (range 2.5-9.7%) and 2.7% (1.6-5.7%), respectively, both of which were significantly lower than that in LT recipients (9.0% [4.4-16.2%], p=0.01); however, there was no significant difference between KT recipients and healthy controls.
We further compared the median frequencies of Tregs in patients with different underlying diseases. There were no significant differences based on the underlying disease in KT patients (Fig. 1B). However, LT patients showed different levels of Tregs depending on their underlying chronic liver disease. The highest levels were observed in patients with chronic hepatitis B and alcoholic cirrhosis (both groups p<0.001 compared with healthy controls) (Fig. 1C).
The change in frequency of Tregs after transplantation
In kidney transplant recipients, the frequency of Tregs decreased significantly after transplantation. After transplantation, the median frequency of circulating Tregs was 2% (1-3.6%) at one week, 1.6% (0.5-3.3%) at two weeks and 2.5% (1.7-3.7%) at eight weeks (all p<0.001 compared with those before transplantation) (Fig. 2A). The frequencies of circulating Tregs after LT showed a similar pattern but the differences did not reach statistical significance when compared with those before transplantation (Fig. 2B).
Association between frequency of Tregs and clinical parameters
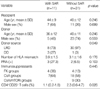
Fig. 3 shows the association between the frequency of circulating Tregs and clinical parameters. The number of HLA mismatches, donor origin, related vs. nonrelated donor, the presence of panel-reactive antibodies and allograft dysfunction were not correlated with the frequency of Tregs (Fig. 3A-E). Infectious complications such as BK virus and cytomegalovirus infection also did not lead to any significant changes in the level of Tregs (Fig. 3F, G). Only patients with subclinical acute rejection in protocol biopsies had significantly decreased frequencies of Tregs compared with those with no detectable rejection (1.1% [0.2-1.8%] vs. 2.3% (0.6-4.7%), p=0.026) (Fig. 3H). So we analyzed these clinical parameters in recipients in whom protocol biopsies were performed (n=42) (Table 2). There were no significant differences between the two groups, except for donor source. The patients with SAR showed high percentage of deceased donor compared with patients without SAR (27% vs. 3%, p=0.049).
The influence of immunosuppressants on the frequency of Tregs
Fig. 4A-C shows the influence of different immunosuppressants on the frequency of Tregs. The frequency of circulating Tregs in the FK groups was higher than other groups before transplantation (p<0.05) but significantly decreased after renal transplantation (p<0.05). Similar finding was observed in the CsA group. However, the mTOR group did not show any significant difference of circulating Tregs before and after transplantation. Frequencies were increased at eight weeks after transplantation but the difference did not reach statistical significance.
We further evaluated whether the blood concentration of the calcineurin inhibitors (CNIs), CsA and FK506, affected the frequency of circulating Tregs. The patients with high FK506 levels (≥10 ng/mL) had lower levels of Tregs than those with low FK506 levels (<10 ng/mL) (Fig. 4D); however, the blood levels of CsA did not affect the level of Tregs (Fig. 4E).
IL-10 ELISPOT assay and Tregs
To explore whether the frequency of IL-10-secreting cells determined by ELISPOT assay was related to the frequency of Tregs, we performed an IL-10 ELISPOT assay in all kidney transplant patients. The median frequencies of IL-10 secreting cells, as determined by ELISPOT, were 95 (17-177), 12 (0-92), 211 (16-345) and 75 (34-118) spots per 200,000 peripheral blood lymphocytes (spots/PBLs) before transplant and at one, two and eight weeks after transplant, respectively. The frequency of donor-specific IL-10 spots was not correlated with the frequency of circulating Tregs before or after transplantation. In addition, there were no differences in the frequencies of donor-specific IL-10 spots between patients with and without subclinical acute rejection after KT (12.5 [0-95] vs. 7 [0-67], 69 [16-188] vs. 75 [24-118], 121 [8-230] vs. 454 [454-454] spots/PBLs at one, two and eight weeks after transplant, respectively).
DISCUSSION
The results of our study demonstrate that the frequency of circulating Tregs during the early posttransplant period in renal transplant recipients is affected by the type of immunosuppressant treatment and associated with subclinical acute rejection. This finding suggests that circulating Tregs may be used as a surrogate marker for assessing immune status of renal transplant recipients during the early posttransplant period.
The frequency of Tregs in patients with ESRD was not significantly different from that in healthy controls (12), but lower than that in patients with chronic liver diseases. The reason for differences in frequency of Tregs between ESRD and chronic liver diseases is unclear, but it may be related to the underlying disease and organ specificity. Even in patients with chronic liver diseases, frequencies of circulating Tregs were different according to etiology: patients with chronic Hepatitis B or alcoholic cirrhosis had higher frequencies of circulating Tregs than did those with other liver diseases (13, 14). This finding suggests that an altered immune response due to Hepatitis B virus infection or alcohol may increase the Tregs frequency.
We found that the frequency of circulating Tregs was significantly decreased after kidney transplantation but not after liver transplantation. This discrepancy between two organs is not fully understood, but it may be explained by organspecific immunity between kidney and liver. It is generally accepted that the liver transplant recipients have less immune response (less acute rejection and more immune tolerance) than kidney transplant recipients (15). This finding suggests that higher frequency of circulating Tregs in liver transplant recipients may be related to the less immune response. Another consideration is the dose and type of immunosuppressants. In our study, liver transplant recipients received less immunosuppression (lower dose of immunosuppressants and the smaller number of anti-CD25 antibody) than patients of kidney transplantation. Therefore, less immune suppression in liver transplant recipients may be partly responsible for higher frequency of circulating Tregs.
To evaluate whether clinical parameters affect the frequency of Tregs, we evaluated the immunologic factors (the number of HLA mismatches, donor origin, related vs. nonrelated donor, presence of panel-reactive antibodies and acute rejection), infectious factors (BK virus and cytomegalovirus) and allograft function (Presence of allograft dysfunction). The results of our study revealed that the frequency of circulating Tregs has no significant association with these clinical parameters except subclinical acute rejection which showed low frequency of Tregs. This finding was consistent with recent reports that showed decreases in circulating Tregs accompany allograft rejection in pediatric liver allograft recipients, and the frequency of peripheral circulating Tregs was significantly decreased after the development of acute rejection in liver transplantation (16, 17). The direct relationship between circulating Tregs and acute rejection is not fully understood in clinical practice, but animal study showed that transfer of Tregs from long-term tolerant mice to allografted mice can prevent rejection of transplanted allogeneic pancreatic islets and skin (18, 19). Therefore, the frequency of circulating Tregs may be used as a surrogate marker for predicting subclinical acute rejection during the early posttransplant period.
The activation of Tregs depends on the engagement of the T-cell receptor and the presence of IL-2 signaling (20, 21). Therefore, CNIs or anti-CD25 antibody may prevent the generation and maintenance of Tregs by blocking IL-2 signaling or receptor (22). Indeed, CNIs decrease FoxP3 mRNA and protein expression in vitro (23, 24) and reduce the number of peripheral blood Tregs in renal transplant recipients (25). The frequency of circulating Tregs decreased in patients treated with CNI or anti-CD25 antibody, but it was difficult to evaluate the influence of immunosuppressant on circulating Tregs separately because all patients received both CNIs and anti-CD25 antibody. However, a high blood concentration of FK506 (≥10 ng/mL) was closely associated with a lower frequency of Tregs. Therefore, we can at least conclude that number of circulating Tregs is affected by blood level of FK506.
In contrast, mTOR inhibitors selectively expand regulatory T cells in vivo (26). Therefore, it is presumable that the patients receiving mTOR inhibitors may have elevated circulating Tregs. In this study, we found that combined treatment of mTOR inhibitors (sirolimus/everolimus) and CsA did not decrease circulating Tregs. This finding suggests that mTOR inhibitors increase circulating Tregs, but direct effect of mTOR inhibitors on number of circulating Tregs needs to be evaluated. Thus, we cautiously conclude that mTOR inhibitors may compensate the decreased circulating Tregs caused by CsA.
IL-10 is required for the generation and suppressor functions of Tregs (6, 27). Boogaardt et al. (28) reported that more IL-10 producing cells were found in patients with a stable graft function than in those with rejection. Therefore, we expected that the frequency of Tregs would have a close association with the frequency of IL-10 producing cells; however, our study did not find any significant correlation between these two factors. The reason for this lack of association between IL-10 producing cells and Tregs is not clear, but it may be related to the small proportion of circulating Tregs in the ELISPOT assay. Further evaluation with selected Tregs may be needed to define the association between circulating Tregs and IL-10.
It is widely accepted that Tregs play a pivotal role in tolerance induction (7). Therefore, an increase in circulating Tregs may be beneficial to the grafted kidney in terms of immune tolerance. The results of our study revealed that the frequency of circulating Tregs is significantly reduced by strong immunosuppressants such as CsA or FK506, and that a high blood concentration of FK506 further reduced the frequency of circulating Tregs. The decrease in frequency of Tregs seen at one and two weeks after renal transplant gradually disappeared by eight weeks after transplant. This finding suggests that high doses of CNIs at the time of transplantation prevent the development of Tregs (29) and that tapering of CNI may prevent a further decrease in circulating Tregs. Thus, treatment with CsA or FK506 in the early posttransplant period should be used cautiously and high doses of CNIs should be avoided because it may inhibit the development of immune tolerance. Further evaluation of the long-term effect of CNIs on circulating Tregs and the optimal frequency of circulating Tregs during the early transplant period in kidney transplantation is needed.
One could argue that FK506 may increase subclinical acute rejection by decreasing circulating Tregs because the results of our study revealed that a lower frequency of circulating Tregs was associated with subclinical acute rejection. In our center, we use FK506 in immunologically moderate to high risk patients such as those with high numbers of HLA mismatches, nonrelated or deceased donors and in retransplanted recipients. Therefore, these patients have many risk factors for acute rejection and, indeed, the incidence of subclinical acute rejection in protocol biopsies in the FK506 group was not increased compared with CsA groups. Therefore, an association between FK506 treatment and subclinical acute rejection in terms of circulating Tregs may be excluded.
In summary, monitoring of circulating Tregs in peripheral blood is helpful for evaluating the immune status of kidney transplant recipients during the early posttransplant period.




 XML Download
XML Download