

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease is the leading cause of death for patients with end-stage renal disease (ESRD). The increased risk of cardiovascular mortality may be attributable to advanced atherosclerotic vascular changes and left ventricular hypertrophy (1). The previous epidemiological and clinical studies have shown that damage to large arteries may be a major factor that contributes to the high rate of cardiovascular mortality for patients with ESRD (2, 3). The increased sclerosis and stiffness of the abdominal aorta reflect early atherosclerosis and this is significantly correlated with coronary arteriosclerosis (4, 5). Blacher et al. (3) reported that aortic stiffness predicts all-cause mortality and cardiovascular mortality in patients with ESRD, and this suggests that arterial wall stiffness may be a good predictor of cardiovascular mortality in ESRD patients. Therefore, evaluating the arterial pathophysiologic characteristics is critical for the early detection and prevention of atherosclerosis.
Pulse wave velocity (PWV) represents a valid noninvasive method for assessing asymptomatic atherosclerosis or arterial stiffness. The elastic properties of the aorta are important determinants of cardiovascular events, and the PWV measured along the aortic pathway is quite clinically relevant (6). Several studies have reported that the PWV was a strong independent predictor of the overall and cardiovascular mortality of hemodialysis patients (6, 7). Left ventricular hypertrophy (LVH) is the most frequent cardiac abnormality and it is a strong, independent risk factor for the cardiovascular morbidity and mortality of dialysis patients. Increased arterial stiffness is associated with an increased left ventricular overload, which may be associated with left ventricular hypertrophy in patients with ESRD (8). These results support the hypothesis that measurement of the aortic PWV could help not only for assessing LVH, but also for predicting cardiovascular mortality. However, the relationship among aortic stiffness, left ventricular hypertrophy and cardiovascular mortality has not been fully evaluated for dialysis patients.
The purpose of the present study was to assess the factors that contribute to aortic stiffness and to investigate whether increased arterial stiffness, as assessed by the aortic pulse wave velocity, affects the cardiac alteration in hemodialysis patients. We also studied the relationship between the aortic PWV and cardiovascular events.
MATERIALS AND METHODS
Patients
A total of seventy two patients with ESRD and who had been on intermittent hemodialysis treatment for more than 6 months at our hospital were included in this study. All the subjects gave us their informed consent after receiving written explanation about the study. Cross-sectionally, we measured pulse wave velocity, and we performed 24 hr ambulatory blood pressure monitoring and echocardiography. We excluded those patients with severe illness such as malignancy, liver cirrhosis, present myocardial, cerebrovascular or peripheral vascular disease, previous history of cardiovascular disease within 6 months prior to study and apparent acute infection.
The patients received hemodialysis treatment 4 hr/session three times a week during the study period. First-use hemophane (GFr12 Plus; Gambro, Tokyo, Japan) was used for hemodialysis. The following characteristics were measured or calculated: age, gender, the body mass index (BMI), the duration of hemodialysis, Kt/V, the presence of diabetes mellitus, the presence of statin use, the number of anti-hypertensive drugs used (angiotensin converting enzyme inhibitor, angiotensin receptor blocker, calcium channel blocker, beta-blocker, alpha-blocker, direct acting anti-hypertensive drug) and the smoking history.
Biochemical assays
Biochemical parameters including lipid profiles were measured by using routine laboratory methods. The serum intact parathyroid hormone (iPTH, the Nicholas immunoradiometric assay) and the serum high-sensitivity C-reactive protein (hs-CRP, Latex Immunoturbidometry) were measured. The level of low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald formula. All the blood samples for biochemical assays were drawn in the morning at the beginning of the dialysis session.
Measurement of the pulse wave velocity
All the measurements of PWV were performed using an applanation tonometer (PP-1000, Hanbyul Meditech Co., Seoul, Korea). The PWV was determined as the difference in travel time of the pulse-wave between two different recording sites and the heart, divided by the travel distance of the pulse-wave form. An electrocardiogram (ECG) was used to determine the start of the pulse-wave. The mean of 10 sec of the tonometer recorded pulse-waves at the femoral and carotid arteries (aortic PWV) was used to determine the arrival of the pulse-wave at the peripheral recording site. The distances were measured as straight lines between the sternal notch and the points of applanation with using a tape measure, with the transit distance defined as the distance from the sternal notch to the femoral artery minus the distance from the sternal notch to the carotid artery (9, 10).
Ambulatory blood pressure monitoring and echocardiography
Twenty four hour ambulatory blood pressure monitoring (24 h-ABPM) was performed between two dialysis sessions with using an ambulatory blood pressure monitor (Oscar oscillometric ambulatory blood pressure monitor, SunTech Medical, NC, U.S.A.). It was programmed to measure the blood pressure every 30 min from 6:00 to 20:00 (daytime) and from 20:00 to 6:00 (nighttime). The 24 h-ABPM variables included the average systolic blood pressure (SBP), the mean arterial blood pressure (MAP), the diastolic blood pressure (DBP), the heart rate (HR) and the pulse pressure (PP). The blood pressure thresholds were 135/85 mmHg (daytime mean blood pressure) or 120/75 mmHg (nighttime mean blood pressure); that is, the average recordings at or over these levels were classified as hypertension. For all the patients, antihypertensive drugs, coronary vessel dilators, anti-platelet agents, lipid lowering agents and erythropoietin were continuously administered during the study.
Two-dimensional echocardiography was performed with the subjects in the left decubitus position (Sonos 5500, Hewlett-Packard, Andover, MA, U.S.A.). A single experience cardiologist, who was unaware of the clinical details of the patients, performed the measurements. The left ventricular mass (LVM) was corrected by the body surface area, and it was expressed as the LVM index (LVMi); the left ventricular end-diastolic volume (LVEDV), interventricular septal thickness (IVST), left ventricular posterior wall thickness (LVPWT), left atrial diameter (LAD) and left ventricular ejection fraction (LVEF) were calculated according the recommendations of the American Society of Echocardiography (11). The LVM was calculated according to the Devereux formula and it was indexed to height2.7 (LVMi). LVH was defined by a LVMi of over 47 g/m2.7 in women or a LVMi over 50 g/m2.7 in men (12).
Statistical analysis
The data is expressed as means±SD. Chi square tests and ANOVA tests were used. The correlation between the variables were tested by Pearson's rank correlation test (r=correlation coefficient). We also used multivariate linear regression analysis to assess the linear associations between the AoPWV and the determinants of the clinical, biochemical and echocardiographic parameters of the study's patients. Cox's proportional hazard regression analysis was used to compare the hazard ratios between the patients with or without cardiovascular events. The survival curves were estimated by the Kaplan-Meier product-limit method and they were compared by the log rank test. Statistical analysis was performed using SPSS soft ware, version 11.0 (SPSS, Inc., Chicago, IL, U.S.A.). A p value of less than 0.05 was considered statistically significant.
RESULTS
Baseline characteristics of the hemodialysis patients
The mean age of the patients at inclusion was 50.4±13.0 yr (range: 26-75 yr) and the mean duration of dialysis treatment was 46.7±33.6 months (range: 8-180 months). Fourty-two patients (58.3%) were men, and 33 of the patients (45.8%) had diabetes. The majority of our patients reported a history of hypertension, with 75% receiving antihypertensive therapy (mean 1.8±1.5 antihypertensive medications). Fifty patients (69.4%) received RAS blockade (angiotensin converting enzyme inhibitor, ACEI or angiotensin receptor blocker, ARB) and 22 patients received statins (30.5%). The mean aortic pulse wave velocity of the patients was 8.09±1.12 m/sec.
Analysis of the aortic pulse wave velocity according to the patient groups
We divided our population into tertiles with respect to their AoPWV value, and then grouped the patients according to the tertiles: the low AoPWV group (the first tertile, AoPWV value <7.4 m/sec, n=24), the middle AoPWV group (the second tertile, AoPWV value 7.4-8.2 m/sec, n=24) and the high AoPWV group (the third tertile, AoPWV value >8.2 m/sec, n=24). Comparison of the clinical and biochemical parameters among groups is shown in Table 1. The mean values of age at inclusion, the serum hs-CRP, the average PP, the average Ao PWV, LVMi and the prevalence of LVH for the high AoPWV group were significantly higher than those of any other group (p<0.05). Likewise, the prevalence of diabetes and statin use showed significantly higher values for the high AoPWV group than those of the low AoPWV group (p<0.05). In contrast, serum albumin was significantly lower for the high AoPWV group compared with that of the low AoPWV group (p=0.02). There were no significant differences between the two groups for gender, BMI, the number of smokers, medication of ACEI or ARB, the duration of dialysis, the adequacy of dialysis (Kt/V), the values of the hematocrit, total cholesterol, triglyceride, LDL-cholesterol, phosphorus, the products of calcium and phosphorus, iPTH, the average MAP, DBP and HR and the echocardiographic parameters, except for the LVMi.
Association between AoPWV and clinical parameters
Pearson's correlation test was performed to examine the relationships between AoPWV and the clinical parameters. The AoPWV value was positively correlated with age (r=0.40, p=0.01), the presence of diabetes (r=0.27, p=0.04), the serum calcium (r=0.31, p=0.02), the hs-CRP (r=0.38, p=0.01), the average pulse pressure (r=0.38, p=0.01), the LVMi (r=0.24, p=0.03) and the LAD (r=0.22, p=0.04), but the AoPWV value was negatively correlated with the serum albumin levels (r=-0.31, p=0.02) and the LVEF (r=-0.26, p=0.03). However, there were no significant correlations between the AoPWV and the other parameters, such as the use of RAS blockade or statin, serum levels of total cholesterol, triglyceride, LDL-cholesterol, phosphorus, the products of calcium and phosphorus, iPTH, the average DBP, MAP, and HR and the echocardiographic parameters, except for the LVMi and the LAD (data not shown). Multivariate linear regression analysis indicated that age (β=0.362, p=0.013) and the average PP (β=0.324, p=0.025) were independently associated with the Ao PWV values (R2=0.297, p=0.001) (Fig. 1) (Table 2).
Cardiovascular outcomes
We followed up the patients for a mean of 46±33 months (range: 12-46 months). A total of 26 fatal or non-fatal cerebro-cardiovascular (CV) events were recorded. Eighteen events were cerebral infarction, five were coronary artery disease (unstable angina 3, myocardial infarction 2) and three were cerebral hemorrhage. Two patients had both unstable angina and cerebral infarction.
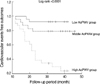
Univariate Cox proportional hazards analysis showed that age (p=0.016), the serum albumin (p=0.012), the hs-CRP (p=0.022), the average MAP (p=0.033), the average PP (p=0.001), the AoPWV (p=0.001), the LVMi (p=0.024), the LVEF (p=0.001), the LAD (p=0.003) and the LVESV (p=0.003) were significant predictors of CV events. There was not statistical significance in gender, the time on dialysis before inclusion, the presence of diabetes and the average systolic blood pressure. On the multivariate Cox proportional hazards analysis, the AoPWV (p=0.018) and the average PP (p=0.004) remained the significantly independent predictors of CV outcomes (Table 3). Fig. 2 shows the probability of cardiovascular survival according to the AoPWV groups. Comparison between the survival curves was highly significant (log-rank test, chi square=26.5; p<0.0001).
DISCUSSION
Increased arterial stiffness (reduced arterial compliance) seems to have a critical role in the development of high SBP, a widened PP, left ventricular work overloading and hypertrophy and increased CV mortality (13). The mechanisms for increased arterial stiffness in patients with uremia are not fully understood, but they may include fluid overloading, arterial calcification, inflammation, activation of sympathetic nervous activity, activation of the renin-angiotensin system and increased lipid oxidation and oxidative stress. Structural changes in the large arteries are characterized by dilation, wall thickening and calcifications, and these changes are more frequent in ESRD patients (13).
In this study, the AoPWV was significantly associated with age, the presence of diabetes, the hs-CRP, the serum albumin and calcium and the average PP. These findings are consistent with several previous studies (14, 15). In our study, the independent parameters that were entered into the multivariate linear regression analysis of the AoPWV were age and average PP.
The aortic PWV increases with age and the systolic blood pressure, and so it should be considered accordingly. Previous studies on ESRD patients have shown that arterial stiffness is enhanced independently of age and the systolic blood pressure (16). Our data is consistent with several reports showing a significant association between age and aortic stiffness (13, 16). Age is known to be a more important contributing factor to the central (aortic) PWV than to the peripheral (brachial) PWV (6, 17). Age also seems to plays a more critical role for aortic stiffness in the older dialysis population than in the relatively young dialysis population. Although a previous study by Covic et al. (13) failed to demonstrate a significant correlation between age and aortic stiffness, the mean age of our patients was higher than that of their study (50.4±13.5 vs. 42.6±11.2 yr, respectively). Our results failed to show a relationship between AoPWV and the average (p=0.07). The majority of our patients receiving hemodialysis reported a history of hypertension, with 75% receiving antihypertensive therapy. So, the effect of drugs for the treatment of hypertension should be considered when interpreting our results.
It is well known that most patients with ESRD have LVH or systolic dysfunction. Some studies reported that an increased AoPWV has been observed in ESRD patients and this is directly related to the magnitude of the LVH (18, 19). The increased arterial stiffness raises the systolic blood pressure and pulse pressure, thereby causing an increased left ventricular afterload and altered coronary perfusion. We demonstrated a weak, but significant correlation of AoPWV with the LVMi and LVEF in hemodialysis patients, which suggests that arterial stiffness may contribute to the development of LVH in these patients. However, we did not show an independent association between AoPWV and the LVMi on the multivariate linear regression analysis.
A previous study has shown that the increased aortic PWV was predictive of adverse cardiovascular outcomes, indicating that arterial stiffness is not only a marker of established and more advanced arterial changes, but it is also a risk factor that contributes to the development of cardiovascular disease (20). The studies of hemodialysis patients have reported that the PWV independently predicted all-cause and cardiovascular mortality (7). The present study supports the previous findings of PWV as a predictor for cardiovascular mortality (6, 9). In this study, after adjustment for all the other cardiovascular risk factors (including age, gender, the average SBP and the presence of diabetes), the AoPWV and the average PP were significant independent predictors of the cardiovascular outcome. For each PWV increase of 1 standard deviation, the cardiovascular events hazard ratio was 1.73 (95% CI, 1.10 to 2.72). Another important finding in our results is that the AoPWV remained independent predictors of cardiovascular events in spite of the presence of influence by an important confounder, the LVMi. The results of a previous study by Blacher et al. (6) showed that the PWV was a strong predictor of survival for ESRD patients on the multivariate Cox proportional analysis with using all the variables, including the LVH. As is well known, an increased LVMi and LVH are potent predictors of cardiovascular mortality for hemodialysis patients. The reason why the present result was revealed is unclear. A possible explanation of this result is that most of the cardiovascular events in our study were cerebrovascular accidents, and mainly cerebral infarction. Eighteen cardiovascular events (69.2%) were cerebral infarction in our population, and only five (19.2%) were cardiac events. Aortic stiffness is vascular change and this is associated with atherosclerosis and arterial calcification. So, we think that prior to cardiac alteration, arterial stenosis or occlusion more frequently develops before cardiac events occur.
Another interesting finding in the present study is that the average PP had significant correlation with the AoPWV and it was an independent predictor of cardiovascular events. Zureik et al. (21) insisted that the increased pulse pressure causes hemodynamic barotrauma to the vascular wall, which causes endothelial damage and inflammation, and the final result is atherosclerosis or arterial stiffness. Furthermore, Safar et al. (14) have shown that the carotid PP (a close surrogate of the aortic PP), the ratio of the brachial PP to the carotid PP and the PWV are all significant independent predictors of all-cause mortality. These results provide evidence of the clinical utility of measuring the PP together with the PWV in hemodialysis patients for predicting cardiovascular morbidity and mortality.
Our study has several limitations. First, the size of this study was relatively small and the follow up period was shorter than that of other studies. As was previously described, we failed to show the association between AoPWV and the average SBP which is an important contributing factor for aortic stiffness. We think that a large cohort and a long period study are needed to prove the correlation of both parameters. Second, in our results, we did not find enough cardiac morbidity such as atrial fibrillation, congestive heart failure or systolic dysfunction. This may be one of the reasons why the LVMi did not remain an independent predictor of cardiovascular events. Third, the patients' treatment was not standardized during the follow-up period. Our study did not show a significant correlation of AoPWV with the lipid profiles or calcium and phosphorus levels, which are important for arterial calcification or as atherosclerotic risk factors. In addition, although the prevalence of the use of statin was higher in the high AoPWV group than that in the low AoPWV group, we failed to demonstrate the association between AoPWV and the use of RAS blockade or statin. Previous studies reported that RAS blockades or statin improve arterial stiffness in type 2 diabetes or essential hypertension (22, 23). Although it is practically impossible to do in such complex patients who are followed for long periods of time, the effect of drugs on the treatment for hypertension with RAS blockade, for dyslipidemia with statin or for the calcium and phosphorus metabolism should be considered in this kind of study. Fourth, in this study, we evaluated arterial stiffness of patients with aortic PWV and brachial PP. Recently, two highly reproducible markers of aortic stiffness-aortic PWV and augmentation index (AIx)-have been shown to be strong CV morbidity predictors for patients on haemodialysis (24). The AIx is the one of the methods for arterial stiffness using arterial wave reflections and provides a measure of systemic arterial stiffness (25, 26). There are some reports demonstrated that AIx is more reliable method for evaluating arterial stiffness than PWV, and it can be affected by multiple factors such as blood pressure, age, gender, height and heart rate (27, 28). On the other hand, peripheral pulse pressure does not always predict central pulse pressure, which is important because central, not brachial artery, pressure best defines left ventricular workload and, thus, an important and independent predictor of cardiovascular mortality. Central PP (carotid artery or ascending aorta) has shown an independent predictive value for all-cause mortality in patients with end-stage renal disease and in the hypertensive patients (29). But some studies reported that aortic PWV is highly correlated with AIx, and a decline in endothelial function is associated with increased large artery stiffness, wave reflections, and central pulse pressure (30, 31). So, we think that further study including PWV, AIx and central PP concomitantly for evaluating aortic stiffness should be needed in dialysis population.
In conclusion, the present study shows that the AoPWV is independently associated with age and pulse pressure, and it is a significant predictor of the cardiovascular outcome for patients who are on maintenance hemodialysis. Our results support the hypothesis that measurement of the aortic PWV could help not only for risk assessment, but also for creating risk reduction strategies by monitoring the arterial stiffness of patients who are under different drug regimens.




 XML Download
XML Download