

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Dialysis patients have a high incidence of cardiovascular morbidity and mortality (1, 2). Vascular calcification (VC) in hemodialysis (HD) patients was associated with increased stiffness of the artery and has already known to be related to cardiovascular disease and cardiovascular mortality (3-5). The simple VC score of plain radiographic films of the pelvis and hands was independently associated with coronary artery disease and peripheral arterial disease at the end of the follow-up (6). There are two types of VC on the plain radiograph, arterial medial calcification and arterial intimal calcification which has irregular and patchy distribution. The presence of medial artery calcifications on the plain radiograph which is more common in dialysis patients than in the general population, is a powerful and independent prognostic marker for all-cause and cardiovascular mortality in chronic HD patients (7, 8). Typical linear railroad-track type (angiography like) calcifications on the plain radiograph that outline the vessel walls are considered as medial artery calcification which is differentiated from intimal calcifications (7). Medial artery calcification of dorsalis pedis artery on the plain radiography of feet is also one of peripheral artery vascular calcifications such as vascular calcification of hands.
Maintenance dialysis patients have a reverse association with some traditional risk factors; body mass index (BMI), hypercholesterolaemia and hypertension reduced the relative risk of death in epidemiological studies (9-11). In fact, dialysis patients have specific non-traditional risk factors; inflammation, malnutrition, oxidative stress, and abnormal mineral metabolism are other important risk factors for vascular disease (12). In general, oxidized low density lipoprotein (ox-LDL) cholesterol is closely associated with the inflammatory process in vascular atherosclerotic lesions (13, 14) and inflammatory marker, C-reactive protein (CRP), is a stronger predictor of cardiovascular events than low density lipoprotein (LDL) cholesterol (15). Plasminogen activator inhibitor-1 (PAI-1) is also linked to vascular inflammation and atherosclerosis (16). Thus, CRP, PAI-1 and ox-LDL have a high possibility of relation with VC which is risk factor of cardiovascular morbidity and mortality in dialysis patients. The present study was designed to find factors related with medial artery calcification on the plain radiography of feet by comparing CRP, PAI-1 and lipid profile including ox-LDL and to elucidate associations among these factors in HD patients.
MATERIALS AND METHODS
Patients
We recruited a total of 48 HD patients (male: 24 patients, diabetes: 14 patients) from Dong-A University dialysis center and a neighboring local dialysis center. Patients with HD duration of less than 6 months, patients with a catheter as vascular access, history of active infection within 3 months, malignancy and chronic liver disease were excluded. The mean age of the patients was 56.3±11.5 yr and the mean duration on HD was 77.1±54.1 months. Enrolled HD patients received regular HD thrice weekly. Bicarbonate-based dialysate and polysulphone dialyzers (Fresenius, Bad Homburg, Germany) were used. Informed consent was obtained in accordance with the guidelines set forth by the Declaration of Helsinki. We defined medial artery calcification on the plain radiograph of feet as vascular calcification. We reviewed medical history and records by chart review and interview. Coronary artery disease (CAD), cerebrovascular accident and peripheral artery disease (PAD) were defined as cardiovascular disease (CVD). We defined CAD based on the records of myocardial SPECT scan, echocardiography or coronary angiography. Patients with a history of lower extremity amputation caused by PAD, stenosis of peripheral artery on the color doppler ultrasonography or present ulceration and necrosis of the foot were defined as PAD. We reviewed current medications and checked blood pressure of the enrolled patients in the sitting position before hemodialysis.
Radiography of both feet
Standard radiographs of both feet were taken to determine VC. AXIOM Aristos MX/VX (SIEMENS, Erlangen, Germany) radiographic equipment with digital imaging system was used and exposure condition was approximately 45-50 kVp (4 mAs).
Calcifications that outline the dorsalis pedis artery on the plain radiograph were shown as typical linear railroad-track form like angiography (Fig. 1). VC of this form indicates medial artery calcification. One nephrologist and one radiologist individually decided VC of the dorsalis pedis artery on the plain radiograph without information of patients. Consensus was reached on the interpretation of all radiographs.
Laboratory measurements
Routine laboratory tests such as hemoglobin, blood urea nitrogen (BUN), creatinine, albumin, calcium, phosphate, intact parathyroid hormone (iPTH), CRP and lipid profile were obtained using fasting blood samples. Normalized protein catabolic rate (nPCR), fractional clearance of urea as a function of its distribution volume (Kt/V urea) and BMI were also determined. HbA1c was checked in diabetic patients. PAI-1 was measured by ASSERACHROM® PAI-1 kit (Diagnostica stago Inc, NJ, U.S.A.), oxidized LDL (Mercodia, Uppsala, Sweden) and anti-oxidized LDL antibody (oLAB; Biomedica, Vienna, Austria) was measured by using a commercially available enzyme linked immunosorbent assay kit.
Prehemodialysis blood samples were obtained from the arteriovenous fistula or graft in HD patients. Samples were immediately placed on ice. Plasma and serum were promptly separated by centrifugation and stored at -70℃ until assayed.
Statistics
Data are presented as mean±S.D. except iPTH which is expressed as mean±S.E. Comparisons of unpaired data were performed using Mann-Whitney U test. Correlation analyses were examined by using Spearman test. Differences in frequency were tested using chi-square analysis. Significant variables identified by univariate analysis were entered into a binary logistic regression analysis to identify variables associated with vascular calcification. p values less than 0.05 were considered significant. All statistical calculations were performed with SPSS software, version 12.0 (SPSS Inc, Chicago, IL, U.S.A.).
RESULTS
Comparison of data according to vascular calcification
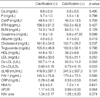
Data are summarized in Table 1 and Table 2. The prevalence rate of VC was 37.5% in these HD patients. VC on the plain radiography of feet was found to be significantly more common in diabetic patients than in non-diabetic patients (66.7% vs. 6.7%, p<0.001). Diabetic HD patients showed significantly shorter HD duration than non-diabetic HD patients (34.5±36.0 vs. 95.0±50.6 months, p<0.001). HD duration was also shorter in patients with VC than in patients without VC. Age, gender, BMI, smoking history, systolic blood pressure, diastolic blood pressure and calcium loads by taking phosphate binder were not significantly different among groups with VC and without VC. History of coronary artery disease and cardiovascular disease were more frequent and pulse pressure was higher in patients with VC than in patients without VC. The percent of patients who had been taking aspirin was significantly higher in patients with VC than in patients without VC. The percent of patients who had been taking angiotensin converting enzyme inhibitors, angiotensin receptor blockers, calcium channel blockers, calcium acetate phosphate binder (94.4% vs. 93.3%), statin and vitamin D was not significantly different among groups with VC and without VC (Table 1). Patients with VC had much more arteriovenous graft as a vascular access compared to patients without VC. Patients with VC showed significantly higher oxidized LDL to LDL ratio and CRP levels, lower high density lipoprotein (HDL) cholesterol than patients without VC. Calcium, phosphate, iPTH, BUN, creatinine, serum albumin, total cholesterol, triglyceride, LDL, ox-LDL, anti-oxidized LDL antibody (oLAB), PAI-1, HbA1c, nPCR and Kt/V urea were not significantly different among groups with VC and without VC (Table 2).
Correlation between ox-LDL/LDL, HDL, CRP, and PAI-1
A negative association was found between ox-LDL and oLAB (r=-0.426, p=0.003). Negative associations were found between HDL and PAI-1(r=-0.375, p=0.009), CRP (r=-0.336, p=0.023) (Fig. 2). A positive association was found between PAI-1 and ox-LDL to LDL ratio (r=0.305, p=0.016).
Logistic regression analysis according to vascular calcification
Significant predictors detecting the presence of VC were diabetes mellitus, history of cardiovascular disease, HD duration, pulse pressure, HDL and ox-LDL to LDL ratio in univariate analysis. History of cardiovascular disease was the only independent factor associated with the presence of VC (odds ratio: 55.71 and 95% confidence interval: 2.75-1130.46, p=0.009) by multivariate analysis including age and gender (Table 3).
DISCUSSION
VC in dialysis patients has been related to diabetes, CVD and increased stiffness of artery (3-5, 8, 17, 18). In our study, history of diabetes, CVD and high pulse pressure were related with the presence of medial artery calcification on the plain radiography of feet, but history of CVD was the only independent factor associated with the presence of VC. Thus we can consider evaluation of CVD if there is angiography like VC of dorsalis pedis artery on the plain radiography of feet in HD patients. A recent report mentioned that coexistence of coronary artery calcification (CAC) and peripheral artery calcification was common particularly in chronic kidney disease patients with diabetes, although VC detected by plain radiograph of foot was not an adequate marker for identifying patients with CAC (19). They checked a standardized plain radiograph of the left foot to determine if there was any calcification of the dorsalis pedis artery, not medial artery calcification.
Ox-LDL is known as a marker of atherosclerosis in HD patients (20). High levels of ox-LDL are associated with calcification of the aortic valve in patients with aortic valve stenosis (21). However, ox-LDL was not involved in coronary artery calcification in HD patients (22). Ox-LDL was not significantly different, but ox-LDL to LDL ratio was significantly different among groups with VC and without VC in our study. Ox-LDL to LDL ratio, an accurate estimation of in vivo LDL oxidation (23), indicates an environment of oxidative stress in HD patients with relatively low LDL levels. Thus, we suggest that the formation of medial artery calcification on the plain radiograph of feet may be affected by oxidative stress. In other aspect, if there are medial artery calcifications of feet, they reflect high oxidative stress condition.
The higher titer of anti-oxidized LDL antibody in females and young persons had a negative association with atherosclerosis (24) and anti-oxidized LDL antibody was independently inversely associated with arterial wall thickness in HD patients (25). Ox-LDL had a reverse relationship with anti-oxidized LDL antibody in our HD patients. This result supports the anti-atherogenic role of anti-oxidized LDL antibody. But there is no evidence that anti-oxidized LDL antibody is related with VC in our study; it requires further study.
HDL was significantly associated with calcification in extra-coronary arteries evaluated by electron beam computed tomography (26). Furthermore, low HDL levels were associated with rapid progression of coronary artery calcification determined by electron-beam computed tomography in HD patients (27). HD patients with VC exhibited significantly lower HDL levels than HD patients without VC in this study. Thus, low HDL which is common in dialysis patients may play a role in the formation of VC on the plain radiograph of feet.
HDL has anti-oxidant and anti-inflammatory properties. The anti-oxidant effect of HDL was shown by inhibition of LDL oxidation in healthy young men (28). In our study there was no association between HDL and ox-LDL but a negative association was found between HDL and CRP as well as HDL and PAI-1, which are important markers of inflammation and atherosclerosis. PAI-1 levels are elevated in dialysis patients with developing atheromatous cardiovascular disease associated with oxidative stress and inflammation (29). A recent report showed that PAI-1 was related with ox-LDL and inflammation in HD patients (30). PAI-1 had a positive relation with ox-LDL to LDL ratio in our study. This result supports that PAI-1 may be linked to oxidative stress. CRP levels were elevated in our HD patients with VC compared to HD patients without VC. Krasniak A et al. (22) reported that CRP was related with coronary artery calcification in HD patients, although CRP was not an independent factor. Finally, these observations suggest that ox-LDL/LDL, HDL, PAI-1, and CRP may be indirectly cross-inked in HD patients who have conditions of oxidative stress and inflammation.
This cross-sectional study has some limitations. The duration of dialysis correlates with calcification in the peripheral arteries (8). But our study showed that HD duration was shorter in patients with VC than in patients without VC. This result is affected by diabetic HD patients, who had shorter HD duration and frequent VC in our study. And cardiovascular calcification was more prevalent in those receiving calcium containing phosphate binders (31). But our cross-sectional study showed that calcium, phosphate, calcium and phosphate product, iPTH, phosphate binder and vitamin D medication was not different among groups with VC and without VC. Thus prospective study will be needed to evaluate the effect of hyperphosphatemia and phosphate binder in HD patients without vascular calcification.
In conclusion, Ox-LDL/LDL, HDL, CRP, and PAI-1 were closely related with one another in HD patients. History of CVD is the most important factor associated with the presence of VC in the feet and low HDL and relatively high oxidized LDL/LDL ratio may affect VC formation on the plain radiography in the feet of HD patients.




 XML Download
XML Download