

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Significant aortic stenosis carries a poor prognosis when associated with congestive heart failure (1, 2), with such patients having an average life expectancy of approximately two years if not treated (3). Although aortic valve replacement represents the only effective treatment, little is known regarding long-term survival and changes in systolic function following surgery after the occurrence of a severe left ventricular dysfunction. The present study examined the surgical outcomes, post-operative left ventricular changes, and the pre-operative predictors of postoperative cardiac death in the patients with significant aortic stenosis and severe left ventricular dysfunction who underwent aortic valve replacement.
MATERIALS AND METHODS
Study populations
The present study included all patients who underwent aortic valve replacement for significant aortic stenosis and severe left ventricular (LV) dysfunction between January 1990 and July 2007 at Asan Medical Center. Significant aortic stenosis was defined as an aortic valve area less than 1 cm2, and severe LV dysfunction as an LV ejection fraction (EF) less than 35%. During the study period, 1,460 patients underwent aortic valve replacement and among these patients, single aortic valve replacement was performed in 688 patients.
Patients were excluded from the study if they were <18 yr old, had double or triple valve surgery, or had more than moderate (>3+/4) aortic or mitral regurgitation according to echocardiography. Patients who underwent concomitant coronary artery bypass surgery or re-operation were included in the present study. The present study was approved by our Institutional Review Board (IRB) of Asan Medical Center, Seoul, Korea. The requirement for informed patient consent was waived by the IRB owing to the retrospective nature of the study.
Follow-up information was obtained from the medical records. If the patient had not been seen in clinic within the previous six months, follow-up information was obtained from telephone conversations between the patients and one of the investigators. When it was impossible to contact with patients, we have referred to the database of the National Health Insurance Corporation to know whether the patients have been dead or not. The mean follow up duration was 58.6 months (range, 0.9-189.1 months).
Echocardiographic methods
Comprehensive two-dimensional and Doppler transthoracic echocardiography was performed in all patients pre-operatively. The echocardiographic examinations were performed by one experienced observer. The left ventricular mass (g) was calculated as 1.04 ([LVID+PWT+IVST]3-LVID3)×0.8+0.6, where LVID is the internal dimension, PWT is the posterior wall thickness, and IVST is the interventricular septal thickness. Left ventricular ejection fraction (%) was calculated as stroke volume in percent of end-diastolic volume. Aortic valve hemodynamic data were assessed using standard methods, and the aortic valve area (AVA) was calculated with the continuity equation: AVA= (LVOT area X LVOT TVI)/aortic TVI, where LVOT is LV outflow tract and TVI is time-velocity integral. Immediate postoperative study was undertaken using echocardiography at 1 week after surgery. Echocardiograph examinations were possible at more than 6 months postoperatively in 31 patients, and the mean interval from surgery to the final postoperative echocardiography was 26.0 (0.1-130.2) months.
Surgical procedure
All patients underwent aortic valve replacement using mechanical or tissue valves. Bentall's operation was performed in one patient with a mechanical valved-conduit. The patient who underwent Bentall's operation was diagnosed with infective endocarditis and underlying aortic stenosis. Destruction was so severe and involved aortic annulus and aortic wall, so extensive debridement was required and then aortic root replacement was necessary. The type and size of the aortic prosthetic valve, concomitant coronary artery bypass graft surgery and the aortic cross clamp and cardiopulmonary bypass duration were recorded.
Statistical analysis
Data are expressed as mean±standard deviation for continuous variables, and as numbers with percentage for categorical variables. Paired and unpaired Student's t tests were performed to determine intragroup and intergroup differences between mean values for continuous variables, as appropriate. Changes in post-operative echocardiographic findings were analyzed using repeated measures ANOVA. The overall survival was estimated using the Kaplan-Meier method. Risk factor analysis for cardiac-related death was performed using Cox-regression analysis. A P value <0.05 was considered to indicate a significant difference. SPSS software 14.0 (Korean version; SPSS, Inc, Chicago, IL, U.S.A.) was used for statistical analysis.
RESULTS
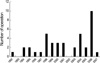
Forty-one patients were identified, and the baseline clinical data are summarized in Table 1. The number of operation per year was described (Fig. 1). The pre-operative mean EF and mean aortic valve area were 26.7±6.1% and 0.54±0.2 cm2, respectively. Mean transvalvular gradient was 48.2±17.4 mmHg. Pulmonary artery hypertension defined as estimated right ventricular systolic pressure more than 50 mmHg was present in 16 patients (45.7%). Pre-operative electrocardiogram showed to be sinus rhythm in 31 patients and atrial fibrillation in 10 patients (24.4%). All patients showed significant symptoms such as dyspnea (n=38), chest discomfort or pain (n=14), and syncope (n=2). Aortic valve pathology was degenerative change (n=26), rheumatic cause (n=1), bicuspid aortic valve (n=13), or infective endocarditis (n=2). All patients underwent either simple aortic valve replacement (n=40) or Bentall's operation (n=1) (mechanical: 23, tissue: 18). The mean valve size was 22.4±2.2 (19-29) mm. Five patients received 19 mm valves (2 St. Jude Medical bileaflet mechanical valves, 1 Hancock II valve, 1 Magna valve, and 1 Carpentier-Edwards pericardial bioprostheses), 14 patients received 21 mm valves (6 St. Jude Medical bileaflet mechanical valves, 1 St. Jude Medical regent valves, 2 MIRA valves, 4 Carpentier-Edwards pericardial bioprostheses, and 1 Biocor valve), 13 patients received 23 mm valves (5 St. Jude Medical valves, 5 Carpentier-Edwards bioprostheses, 1 Hancock valve, 1 MIRA valve, and 1 Top-Hat valve), and 7 received 25 mm valves (2 St. Jude Medical valves, 3 Carpentier-Edwards bioprostheses, 1 TEKNA valve, and Carbomedics valve). One patient each received a 27 mm valve and a 29 mm valve. Combined operations were coronary artery bypass surgery (n=8), ascending aorta wrapping or replacement (n=7), Maze operation (n=1), and patent foramen ovale closure (n=1). Mean cardiopulmonary bypass (CPB) time and aorta cross-clamping (ACC) time were 135.6±56.6 min and 85.6±35.1 min, respectively.
In-hospital mortality occurred in one patient (1/41, 2.4%) who was a 65-yr-old male diagnosed with aortic stenosis and infective endocarditis, and who had an LV EF of 19% and an aortic valve area of 0.43 cm2. While that patient underwent aortic valve replacement with a Carpentier-Edwards pericardial valve, sepsis caused by infective endocarditis was not treated, and the patient ultimately died. Post-operative complications occurred in 7 patients, such as permanent pacemaker insertion due to complete atrioventricular block (n=1), mediastinitis (n=1), post-operative bleeding (n=2), frequent ventricular fibrillation (n=1), acute renal failure (n=1), wound infection (n=2), and infective endocarditis (n=1).
Echocardiograms performed immediate post-operation showed improvement in LV EF, LV mass, LV diameter, and LV volume compared to pre-operative findings (Table 2). During the follow-up period, LV ejection fraction, LV diameter, and LV mass improved dramatically up to 6 months post-operatively, at which point they remained stable (Fig. 2).
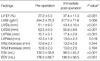
Functional recovery of >10% in the left ventricle was observed in 15 patients (Table 3). Those patients differed from patients with <10% left ventricular recovery in terms of aortic valve area (P<0.026) and left ventricular systolic posterior wall thickness (P<0.021). Pre-operative LV mass was greater in patients who recovered more effectively.
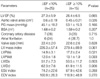
Late death occurred in 12 patients. Of those, 11 patients died due to cardiac-related problems (late death due to unknown etiology was regarded as a cardiac death). Analysis of risk factors for cardiac-related death were performed on patient demographics (age, sex, diabetes mellitus, systemic hypertension, chronic renal failure, and so on), preoperative cardiac function, LV dimension or wall thickness, presence of atrial fibrillation or pulmonary hypertension, NYHA functional class III or IV, emergency operation, combined coronary artery disease, and operative variables (CPB time and ACC time). Univariate analysis showed pre-operative atrial fibrillation (P=0.041) to be a risk factor for cardiac related death. Multivariate analysis showed pre-operative atrial fibrillation, NYHA FC IV, and LV systolic posterior wall thickness to be significant risk factors for cardiac-related death (Table 4). Overall survival rates at 1 yr, 5 yr, and 10 yr were 85.4±5.5%, 72.9±7.5%, and 51.6±12.0%, respectively.
DISCUSSION
Aortic stenosis may be caused by degenerative calcification, congenital malformation, or rheumatic fever. Severe aortic stenosis is defined as an aortic valve area less than 1.0 cm2 (4). Patients with aortic stenosis and left ventricular dysfunction usually improve after surgical treatment of afterload mismatch (5, 6). However, patients sometimes present with severe aortic stenosis and severe left ventricular dysfunction, which leads to concerns over the post-operative state and long-term outcomes.
Advanced patient age, poor preoperative LV function, NYHA class IV symptoms, concomitant coronary artery disease, severe pre-operative renal dysfunction, active endocarditis, female gender, emergency or salvage operation, and previous aortic valve replacement have been associated with increased surgical mortality in several series (5-7). LV dysfunction is an uncommon consequence of aortic stenosis (about 5% of patients), and atrial fibrillation also occurs in only 5% of patients with aortic stenosis (8). In the present study, 10 patients (24.3%) showed atrial fibrillation, indicating that patients with severe LV dysfunction tend to have atrial fibrillation more frequently. The hospital mortality rate in such patients is reported as 8-10.9% (6, 7, 9). In the present study, the in-hospital mortality rate was 2.4% (1/41), and this is an acceptable result compared with other reports. The estimated five year survival of the population after AVR was 72.9% and similar to other reports (6).
Collinson et al. reported that there was a more rapid improvement in LV function following aortic valve replacement with a stentless prosthesis in patients with poor left ventricular dysfunction (10, 11). Improvements in those receiving stented valves appeared delayed, although there were no differences between the groups in terms of LV function or mass at follow-up. Conversely, others reported that they were not able to detect significant differences between stentless and stented valve groups in terms of hemodynamic performance and regression of left ventricular mass (12, 13). In the present study stented prosthetic valves were only used. The present study found a significant improvement in LV EF, LV mass, and LV dimension after the immediate post-operative echocardiogram, which was usually performed at 1 week post-operatively. It was reported that LV mass and functional recovery was complete at 1 or 1.5 yr, and that pre-operative LV function was related to normalization of the LV mass index (14-17). Despite the present study involving patients with severe LV dysfunction, LV function improved dramatically, with most of this improvement occurring in the first 6 months post-operatively.
Functional recovery of >10% in the left ventricle was observed in 15 patients (Table 3). Those patients differed from patients with <10% left ventricular recovery in terms of aortic valve area (P<0.026). Therefore, it could be said that patients with a smaller aortic valve area appeared to have a greater chance of functional recovery after reduction of afterload (18).
Multivariate analysis showed pre-operative atrial fibrillation and NYHA FC IV to be significant risk factors for cardiac-related death. In the present study, the maze operation was done in only one patient (among ten patients with atrial fibrillation), so the further study would be necessary to assess the impact of maze operation in these patients for the survival.
It is generally desirable to avoid using of 19 mm prosthetic valves due to the risk of patient-prosthesis mismatch. The 19 mm valve was used in 5 patients, none of whom experienced cardiac-related death during the follow-up period. This finding is consistent with those of others showing that valve type or size was not related to normalization of LV mass index (19).
This study had several limitations, most of them being inherent to the retrospective analysis of a single center. Firstly, the sample size was relatively small because severe aortic stenosis and severe LV dysfunction are rarely concomitant. Secondly, our choice of a 35% in LV EF as a cut off value of severe LV dysfunction may seem arbitrary. This choice was based on the practically used criteria in our institute. Thirdly, echocardiographic follow-up at more than 6 months was possible in only 31 of 41 patients, while immediate post-operative echocardiography was possible in 40 patients.
In conclusion, the present study found that operative mortality in patients with significant aortic stenosis and severe LV dysfunction was acceptable. Changes in LV function, LV mass, LV volume, and dimension were highly predictable. LV mass regression, functional recovery, and ventricular volume improvements were progressive processes that occurred soon after surgery and were mostly completed at 6 months. Pre-operative predictors for cardiac-related death were pre-operative atrial fibrillation and NYHA FC IV according to the multivariate analysis. The data indicate that aortic valve replacement should be considered more positively even though patients had significant aortic stenosis combined with severe LV dysfunction. Further study would be necessary to assess the impact of maze operation in patients with the significant AS with severe LV dysfunction combined atrial fibrillation.



 XML Download
XML Download