

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Twin to Twin transfusion syndrome (TTTS) is one of the major complications of monochorionic twin pregnancy and it accounts for 15-17% of overall perinatal mortality. Less than 1% of total twin pregnancy is attributable to monochorionic twin pregnanacy and 10-17% of these twin pregnancies are complicated with twin to twin transfusion syndrome (1). Pathophysiology of twin to twin transfusion syndrome is understood mainly by placental vascular anastomosis. Significant unidirectional deep arteriovenous shunts with or without compensatory bidirectional superficial arterioarterial or venous shunts may exist in the placenta of severe TTTS. Perinatal morbidity and mortality is high as 80-100% when untreated (2). Prognosis is known to be even more fatal especially if the disease is developed at early stage. Recently morbidity and mortality are sharply decreasing thanks to method of isolating or intercepting placental venous anastomosis such as fetoscopic laser coagulation. But this method is only available in centers where all the required equipments are prepared. Due to this limitation, it is not carried out in Korea. The reported treatment methods of TTTS in our country have been serial amnioreduction and amnioseptostomy thus far. However, the treatment results of these methods are not certain in patients with less than 20 weeks of pregnancy periods who are suffering from early severe TTTS. For this reason, the selective feticide is thought to be another treatment of choice for the patients with early severe TTTS whose prognosis is expected to be poor. In this report we first report a case of successful delivery of recipient twin after selective abortion of donor twin using radio-frequency cord ablation in monochorionic twin pregnancy complicated with early severe TTTS at 192 weeks of gestation who showed no improvement after repeated amnioreduction.
CASE REPORT
A 32-yr-old, gravida 2, para 1 woman at 18 weeks of gestation was referred to our hospital by a university medical center because of severe dyspnea accompanying polyhydroamnios. While receiving antenatal care at a local hospital, polyhydroamios was noted at 17 weeks of gestation, and then the patient was transferred to the university medical center. At the university medical center, the patient was treated with amnioreduction. While waiting for the result, the patient complained of severe dyspnea at 18+4 weeks of pregnancy and was transferred to our hospital via emergency department. The patient had no present and past medical history. In addition, the family history was not contributory. This twin conception was spontaneous without any medication or ovulation induction and there was no known significant obstetric or gynecological history of the mother.
A detailed two-dimension high-resolusion ultrasound was done right after admission and showed monochrorionic monoamniotic placenta. Twin had no significant size difference, and the estimated size of the 1st fetus was 18+5 weeks while the 2nd fetus was 17+6 weeks. However, the 2nd fetus was stuck due to the scanty amount of amniotic fluid, and the amniotic fluid index (AFI) of the 1st fetus was 320 mm showing polyhydroamnios. For the relief of patient's symptoms, 1,400 cc of amnioreduction was conducted at the day of admission. And the day after the procedure, the patient was discharged with AFI of 220 mm. Five days after discharge, the patient's dyspnea recurred and the sonographic finding showed AFI increased to 260 mm. The growth of the 1st fetus was normal measuring 19+2 weeks size. But the 2nd fetus was only 17+6 weeks size, presenting the findings of stuck twin. The second amnioreduction treatment was performed and 800 cc of amniotic fluid was removed. However, further reduction couldn't be performed due to intractable pain. Regarding the speed of increasing amniotic fluid, amnioreduction was expected to be performed every week. Complications of amnioreduction and poor outcome of early severe TTTS was explained to the patient and her family. After obtaining informed consent, we decided to perform selective abortion using radiofrequency (RF).
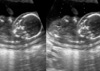
The method of selective abortion using RF ablation was as follows. Just before the procedure, pethidine (Demerol®) 50 mg was injected intramuscularly for emotional stability and pain killing, and prophylactic IV antibiotics was given. Betadine sterilization was done and 2% lidocaine was injected for local anesthesia. Under local anesthesia, 1 mm skin incision was done at the point where the electrode will be inserted. Under the guidance of real-time ultrasonography and color doppler, 17 gauge radio-frequency electrode was carefully inserted to the initiating portion of umbilical cord of the 2nd fetus and radio-frequency ablation was done. Intensity of radiofrequency was estimated by hypoechogenic lesion representing air bubbles which was formed as temperature of tissue rises by radiofrequency (Fig. 1). The RF intensity was increased up to 50 W. A few minutes after the procedure, cardiac arrest of the 2nd fetus was observed. Doppler flow at the cord of 2nd fetus was checked before and after the procedure (Fig. 2). The cord occlusion was successful and there was no blood flow to the 2nd fetus. Mild uterine contraction was noted after the procedure so that tocolytics (ritodrine [Yutopar®], 30 cc/hr) was infused. After the procedure, the patient's symptoms were improved and there was no other complications such as spontaneous premature rupture of membranes or vaginal bleeding. The patient was discharged 4 days after the procedure.
At the follow up ultrasonography performed after the procedure at 20+5 weeks of pregnancy, AFI was increased to 270 mm. The patient complained of dyspnea and 1,900 cc of amnioreduction was done. The patient regularly visited outpatient department and ultrasonography was done to check normal growth and development. and amniotic fluid of the surviving 1st fetus. Growth of the 1st fetus was normal but right mild ventriculomegaly of l.02 cm was noted at 24+6 weeks of pregnancy (Fig. 3). However, it was normalized to 0.9 cm at 28 weeks of pregnancy. Mild oligohydramnios developed after amnioreduction and continued until 24+6 weeks of pregnancy and AFI was measured as 80 mm at 28 weeks of pregnancy. This mild oligohydroamnios status continued until delivery.
At 35 weeks of gestation, the patient was admitted to our hospital with chief complaints of spontaneous premature rupture of membranes and delivered healthy male baby weighing 2.33 kg. Apgar score at the first 1 min was 9 point and 10 point at 5 min. Baby was sent to pediatric department due to prematurity and low birth weight but no other abnormality was found. Selectively aborted 2nd fetus was delivered 5 min after the delivery of first fetus along with placenta. It showed iatrogenic gastroschisis possibly due to radio-frequency ablation to the initiating portion of the umbilical cord of (Fig. 4). Placenta was monochorionic diamniotic, fused type and weighted 430 g. Placenta of selectively aborted fetus was completely infarcted (Fig. 4).
Two days after delivery, the mother was discharged without specific complication and brain sonography of the baby showed normal finding. During the neonatal period baby showed normal growth rate and pattern.
DISCUSSION
TTTS is a serious complication in monochorionic twin pregnancies. This condition is complicated in about 15% of midtrimester monochorionic pregnancies and if untreated, the mortality is reported to be high as 80-100% (1, 2).
Ethiology of TTTS is not fully understood, however, main pathophysiological prerequisite is unequal blood flow via arteriovenous placental anastomosis from the so-called donor to the recipient twin. Due to abnormal interfetal transfusion, the donor becomes progressively hypovolemic, growth restricted and oliguric, all of these lead to oligohydroamnios in this twins amniotic sac. By contrast, the recipient fetus becomes hypervolemic, hypertonic, and might develop congestive heart failure with polyhydroamnios because of the volume overload (3-5). There are two types of placental vascular anastomosis which are superficial and deep. The superficial anastomosis is arterio-arterial anastomosis (AAA) and veno-venous anastomosis (VVA) which appear as a single vessel without interception between the two cord insertions. The problem is arterio-venous anastomosis which anastomose at the villous level and causes arteriovenous connections from the doner to the recipient. This deep connection is responsible for onset of TTTS (6). By contrast, AAA are thought to play a protective role against the development of severe TTTS. Several antenatal diagnostic criteria were described by some authors for TTTS including (1) disparities in weight (>20%) between two fetuses, (2) intertwin hemoglobin difference of >5 g/100 mL (3) other characteristic sonographic features like single monochorionic placenta with same sex, and finding that result from the blood flow discordances such as massive polyhydroamnios (deepest vertical poor >8 cm), distended bladder (signs of polyuria), signs of heart failure or hydrops of the recipient twin and donor twin being stuck due to severe oligo or anhydroamnios (deepest vertical poor <2 cm) (7-9). Doppler sonography shows signs of congestive heart failure (CHF) in severe cases of the recipient and these are negative or revere wave in the ductus venosus, pulsatile umbilical venous flow, tricuspid regurgitation and the signs of decreased venous returns in the donor fetus due to hypervolemia and increased placental resistance (6).
Over the last decades, the choice of treatment for mid trimester TTTS has been the source of considerable controversy. Numerous treatments for TTTS have been introduced, including serial amnioreduction, septostomy, cord occlusion, and selective or non selective fetoscopic laser photocoagulation (10-13). In recent years, the selective fetoscopic laser photocoagulation has become more accepted in the United States. But this method is only available in centers where all required equipments are prepared. Moreover, there are potential limitations such as the difficulty to identify vessel communication in the early 2nd trimester or the difficulty to identify presence of deep vascular arteriovenous anastomosis endoscopically. In that cases there are potential risks of destroying normal cotyledon with resultant placental insufficiency (14). Reported treatment methods of TTTS in our country has been the serial amnioreduction and amnioseptotomy so far, but the treatment results of these methods are not certain in early severe TTTS and with serial amnioreduction, there are complications such as abruption and preterm labor if large volume of amniotic fluid is repeatedly reduced (15, 16). For this reason, in case where the patient with early severe TTTS whose prognosis is expected to be poor, the selective feticide is thought to be another treatment of choice. In case of dichorionic pregnancies, the selective feticide with intracardiac or intrathoracic potassium chloride (KCl) is well established modality, whereas in case of monochorionic twins with vascular communications, the feticide by intracardiac KCl is not suitable because the product may embolize to another fetus (17, 18). So in monochorionic pregnancies, the cord occlusion is a method of choice in current practice. In severe and refractory TTTS, the selective feticide using cord occlusion increases survival rate compared to repeated amnioreduction. The cord occlusion method has been performed with absolute alcohol and enbucrilate gel but the failure rate of these two is reported to be up to 67% (12, 19). So instead of these, recently emerging method is using radiofrequency.
Radio-frequency cord ablation uses high frequency radiowave and causes cell death by protein modification and coagulation necrosis using thermal injury. In vitro study, it is proven that the procedure did not induce any significant temperature rise in surrounding area, which never exceeded 2℃ and might represent a minor risk and RF-induced lesion never exceeded 2 cm in size (20). Although this RF cord ablation occasionally cause complications including mild uterine contraction, acute hemorhage at ablation site, pad burn, and procedure related amniotic fluid leakage, success rate of this procedure is reported as high as 91% (21). Another merit for this procedure is easy accessability. Not like fetoscopic procedure, this procedure needs simple preperation. Furthermore, this is considered to be safe, minimally invasive and transdermal method of effectively interrupting blood flow from donor to recipient fetus, so that it can be the treatment of choice in monochrorionic twin who is suffering from TTTS.



 XML Download
XML Download