

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asbestos was once considered a miracle mineral due to its many favorable characteristics, which include resistance to fire, heat, and corrosion. Asbestos is also strong, durable, flexible, and inexpensive. Asbestos was mined in Korea from the 1930s to the early 1990s (1). In addition, there was a gradual increase in the importation of asbestos in Korea until middle 1990s in response to Korea's rapid economic development (2). Asbestos was commonly used in Korea to make construction materials such as slate; therefore, there is still constant exposure to asbestos even though its use has been banned. In 1993, the first case of mesothelioma in Korea was reported in an asbestos textile worker (3). Since then, mesothelioma cases have been reported continuously, but its pattern differs from that of other countries in that there has been no sharp increase in its occurrence to date (4). In Korea, there has been a series of events related to asbestos over the last 2-3 yr. For example, malignant mesothelioma occurred among several residents who lived near asbestos textile factories in Busan (5), there was a mass outbreak of asbestosis among inhabitants who lived close to asbestos mines (6), and talc containing asbestos which was used to manufacture baby products.
In this article, the general health effects of asbestos are reviewed. In addition, the occurrence pattern of domestic asbestos-related diseases and recent asbestos related events in Korea are examined.
THE USE OF ASBESTOS IN KOREA
Mining of asbestos in Korea began in the 1930s and continued until World War II. In the 1960s, asbestos mining resumed as the asbestos cement industry grew. In the mid-1980s, asbestos mining again ceased because domestic production could not compete with imported one by the low cost. As a result, all asbestos used in Korea has been imported since that time (1). The use of asbestos rapidly expanded in Korea according to the economic growth that occurred in the 1970s. Indeed, asbestos was necessary for the electric power, shipbuilding, and heavy chemical industries to enable heat treatments and the efficient use of energy. However, the major use of asbestos in Korea was in construction materials such as the slate roof tile. In 1997, some forms of asbestos, such as crocidolite and amosite, were banned. Since then, the amount of imported asbestos has gradually decreased (2). Furthermore, all forms of asbestos, including asbestos gaskets and industrial friction materials, have been prohibited in Korea since 2009. Despite the ban on asbestos, Koreans will still be exposed to asbestos remaining in buildings and construction waste.
ENVIRONMENTAL EXPOSURE TO ASBESTOS
In addition to employees who make products that contain asbestos and construction workers who are exposed to asbestos, residents can be affected by environmental exposure to asbestos. Indeed, many countries have reported environmental asbestos exposure, and cases of asbestos related illness are common in Dayao, China, in Kapadokia, Turkey, and throughout the United States and Greece (7-10). Furthermore, asbestos factories and closed or running asbestos mines can provoke great impacts on residents who live nearby.
ASBESTOS REGULATION
In Korea, workers who handle asbestos are covered by two laws: the Industrial Accident Compensation Insurance Act and the Occupational Safety and Health Law. These laws require that the employers direct medical doctors to examine all such workers annually. In May 1997, the manufacture, import, supply and use of crocidolite, amosite and products containing these forms of asbestos were prohibited by the Occupational Safety and Health Law. Additionally, retired asbestos workers who meet certain requirements have been eligible for annual health examinations since 1992. In 2009, the manufacture, import and use of all kinds of asbestos were banned. The occupational exposure limit of asbestos is 0.1 fibers/mL of air and the environmental exposure limit is 0.01 fibers/mL of air.
HEALTH EFFECTS
Ongoing inhalation exposure of asbestos will result in an increasing fiber burden in the lung, thereby increasing the risk for asbestos-related disease. Pleural disease, which is the most common manifestation of asbestos exposure, is subdivided into circumscribed pleural plaques, diffuse pleural thickening, pleural effusion, and round atelectasis (11). Asbestosis is asbestos induced pneumoconiosis, but it has typical characteristics in prognosis and clinical courses. Lung cancer and malignant mesothelioma are known as asbestos related cancer.
Asbestosis
Pulmonary asbestosis is defined as parenchymal fibrosis with or without pleural thickening depending on the intensity of exposure and latency. The fibrosis induces a restrictive lung disease. In general, fibrosis manifests clinically within 20 yr of the onset of exposure. Even short-term exposure for less than one month, if sufficiently intense, can result in asbestosis (11). Asbestosis is usually associated with dyspnea on exertion, bibasilar crackles, and changes in pulmonary function. Cough and chest pain are the chief complaints among asbestos textile workers with asbestosis in Korea, even though their pulmonary function may not decrease severely. Clubbing of the fingers may also occur in advanced cases of fibrosis. Chest radiography are the primary tools to diagnose asbestosis. Upon chest radiography, small and irregular opacities are evident in the mid and lower lung zones. However, some cases of asbestosis cannot be detected by chest radiography; therefore, HRCT is helpful for the diagnosis of patients who do not show definite asbestosis upon chest radiography, but have dyspnea, dry cough, and have developed restrictive changes in their pulmonary function. Pulmonary function changes include a restrictive impairment, with a decreased forced vital capacity (FVC), total lung capacity (TLC), and diffusing capacity (DLCO). It is important to differentiate asbestosis from idiopathic pulmonary fibrosis, congestive heart failure, hypersensitivity pneumonitis, scleroderma, sarcoidosis, rheumatoid lung, desquamative interstitial pneumonia, and other pneumoconioses (11).
Lung cancer
Lung cancer along with mesothelioma is known as asbestos related cancer. In general, asbestos related lung cancer cannot be differentiated from other primary forms of lung cancer. Therefore, it should be examined whether lung cancer accompanies asbestosis when evaluating asbestos related lung cancer. However, some epidemiologic studies have shown that the incidence rate of lung cancer is higher among asbestos workers without asbestosis than among the general population (12). As a result, the following criteria must also be considered to determine if cancer is related to asbestos: cumulative exposure, latency, type of asbestos, and work history. Many countries such as Denmark and the Netherlands apply the Helsinki criteria (Table 1) which include the aforementioned components when determining if cancer is related to asbestos (13).
The first case of lung cancer in asbestos-exposed workers appeared in 1935. At that time, a latency from the onset of exposure to the development of cancers of 20 or more years was observed. Adenocarcinoma is the predominant histologic type but other types such as squamous cell carcinoma, large cell carcinoma, and small cell carcinoma appear in patients with asbestos related cancer (14).
Malignant mesothelioma (MM)
This is a malignancy that occurs in the mesothelial cells of the pleura or peritoneum. Three histological patterns of mesothelioma are recognized: epithelial, sarcomatous, and mixed or biphasic (15). MM is an aggressive tumor that is generally reluctant to current standard treatment modalities including chemotherapy, radiation, and surgery (16). The median survival after diagnosis with MM is less than 12 months. Approximately 80-100% of patients with mesothelioma have a history of exposure to asbestos (17). Although the primary risk factor is asbestos exposure, some studies have suggested that the simian virus 40 may also play a role (18). MM usually develops for more than 20 yr after the onset of exposure to asbestos, although high dose exposure can shorten the latency period. MM patients commonly suffer from chest pain and dyspnea, which prompt initial medical attention. Peritoneal MM presents with signs of ascites and mass effects like distension and pain. The diagnosis is made on the basis of histological examination of cell blocks prepared from pleural fluid or, more commonly, tissue obtained by closed pleural biopsy or thoracoscopy. Immunohistochemical staining is necessary for definitive diagnosis (11).
OCCURRENCE OF ASBESTOS RELATED DEATH AND DISEASES IN KOREA
The resources showing the occurrence of asbestos related disease are the death statistics of the Korea National Statistical Office (KNSO), cancer registry data and mesothelioma surveillance system data (4). Each of those resources has their own strengths and weakness; therefore, conducting a combined analysis of the results of each dataset can be helpful to understanding the occurrence of domestic mesothelioma.
Death statistics of the KNSO
The death statistics of the KNSO can be a good resource for estimation of the mesothelioma incidence rate because its median survival period is 12 months. However, the KNSO has some limitations. For example, MM patients may not necessarily die from mesothelioma itself or the recorded cause of death may not be mesothelioma, even if it was the actual cause. Nevertheless, this resource is very helpful to understanding the occurrence of asbestos related deaths on a national level. According to the KNSO, the mesothelioma death rate among Korean males has increased from 0.65 person/million in 1996 to 1.57 person/million in 2006. In addition, the sex ratio (M/F) of mesothelioma related deaths has increased from 1.4 in 1998 to 3.2 in 2000 (19).
Cancer registry data
Cancer registry data is a very good resource in terms of the clarity of diagnosis. In addition, cancer registry is the most reliable data for estimation of the actual occurrence. However, only the data from 1988 to 2002 were available. The data from 1988 to 2002 show that there were 40-50 cases of mesothelioma in the last 10 yr and that the sex ratio of affected individuals increased from 1.0 in 1993 to 1.8 in 2002. These data also clearly show that the number of cases of mesothelioma has increased (19).
Mesothelioma surveillance system data
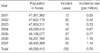
The occupational disease surveillance system is a project designed to provide necessary information to someone who need to use it by collecting, analyzing and evaluating occupational disease data. The mesothelioma surveillance system has been in place since 2000. In Korea, when members of The Korean Society of Pathologists diagnose mesothelioma, they report it to the mesothelioma surveillance center. The advantage of this reporting system is that only cases that have been pathologically confirmed, which is essential to ensuring proper diagnosis of the disease, are collected. It is very important to differentiate mesothelioma from other illness such as metastatic adenocarcinoma of lung cancer; therefore, the certainty of this data is one of its strengths. The surveillance data reveal that the number of cases of mesothelioma has risen rapidly since 2004. Specifically, only 18 cases were reported prior to 1995, but 42 were reported in 2004, 37 in 2005, 53 in 2006 and 55 in 2007. Moreover, an average of 34 cases has been reported annually in this dataset since 2001 (Table 2) (19).
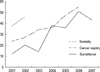
The occurrence trend
These three resources show that the occurrence of MM is increasing gradually (Fig. 1). Considering that asbestos importation reached a peak in Korea in 1995 and that mesothelioma occurrence peaks 25-35 yr after asbestos exposure, domestic mesothelioma occurrence is expected to increase continuously until 2020-2030 (19).
CONSIDERATION OF RECENT ASBESTOS RELATED ISSUES IN KOREA
Occurrence of MM in Busan
A mass outbreak of mesothelioma occurred among residents who had lived near a former asbestos textile factory in Busan. Fourteen cases of MM were reported among residents who lived close to one of the three asbestos factories in Busan and incidence rate of this area was 7-11 times higher than general population (5). This event showed the possibility of the development of the disease in response to environmental asbestos exposure in Korea. The asbestos textile factories were run in Busan and the factory machines came from Japan in the 1970's. It is known that the factories used crocidolite (blue asbestos), which is believed to be most hazardous form of asbestos, during the early years of operation. Additionally, an elementary school is located just 10 meters from the factory; therefore, children who attended that school during the period may develop the disease in the near future. Due to the long latency period associated with asbestos-related illnesses, it is necessary to prepare a long term surveillance of the children.
Asbestosis epidemic near an asbestos mine
In a recent study of the residents of 4 towns in south Chung-Cheong province, where Asia's largest asbestos mine was located, over 50 residents among about 200 were diagnosed with asbestosis. It is suspected that this disease was caused by environmental exposure because most of the individuals diagnosed with the disease did not have a history of working for the asbestos mine. Since there were over 30 asbestos mines in Korea, further studies of the regions in which the mines were located are required. These environmental asbestosis like patients are rarely reported in other countries because asbestosis does not occur without long term exposure to high level of asbestos and asbestos mines are/were located far from village. Therefore, further studies should be conducted to determine the scale of the event. However, facilities are insufficient currently in Korea to analyze asbestos and diagnose asbestos-related diseases, which indicates that more investment in these areas is needed (6).
Talc powder containing asbestos
In April 2009, the Korea Food and Drug Administration (KFDA) determined that 11 talc powder products for babies were contaminated with asbestos, presumably from the manufacturing process. Accordingly, KFDA banned the sales of the identified products and called for a halt in the use of talc in others. Overall, 1,122 drugs and medical goods have been confirmed to contain talc contaminated with asbestos. This event highlights 3 topics that require further studies. First, it is necessary to determine if asbestos-related illness is associated with the use of asbestos-containing baby powder. Second, the risk of asbestos consumed in medicine should be determined. Finally, it is necessary to determine methods of diagnosing asbestos-related illnesses caused by these environmental exposures, as well as compensating the patients, when such illnesses occur. The primary reason for the failure of these 3 issues to be addressed scientifically is that there has not been enough risk communication with the general public. As a result, explanations to the public based on scientific facts failed, and only the fact that asbestos is a carcinogen and that vulnerable individuals such as children and patients with chronic disease were exposed to it was propagated.
It is possible for babies to be exposed to high levels of asbestos through the respiratory tract in response to the use of asbestos-containing baby powder. Although this is a low cumulative level when compared with the results of epidemiologic studies of lung cancer caused by asbestos, it should not be ignored because asbestos is a carcinogen which can cause MM with small amounts. Therefore, the use of such products should be immediately prohibited. However, the hazard of asbestos on individuals exposed through the consumption of medicine is expected to be very low because the medicine contains very small amounts of asbestos and ingested asbestos fibers are poorly absorbed. However, a few epidemiologic studies suggested that asbestos containing drinking water was related to stomach cancer and pancreatic cancer (20, 21). However, contaminated asbestos fibers in the medicines are expected to be extremely lower than those in drinking water. In addition, talc contains non-asbestiform amphibole cleavage as well as asbestos, so, amounts of asbestos may be much smaller than expected (22). Therefore, it is necessary to obtain more accurate and adequate data by evaluating exposure scenarios and conducting animal experiments.
Although workers that develop asbestos-related diseases as a result of occupational exposure can be compensated by industrial accident compensation insurance, there is no way to compensate the patients affected via environmental exposure. Above all, it is not easy to diagnose illnesses caused by environmental exposure. Therefore, comprehensive compensation should be made through an asbestos victim law, which is currently being discussed.
CONCLUSION
Recent asbestos-related events in Korea serve as a momentum for making people be aware of hazard of asbestos. Researchers come to realize risk communication is also important to solve the problem. Building infrastructure for asbestos-related studies, drawing up plan to compensate asbestos victims and laying out environment management plan to minimize asbestos exposure are the most urgent problems to solve at this point of time.

 XML Download
XML Download