

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Microscopic polyangiitis (MPA) is a systemic vasculitis histologically characterized by pauci-immune necrotizing small-vessel vasculitis without granulomatous inflammation. MPA was initially recognized as a microscopic form of polyarteritis nodosa (PAN), accompanied by rapidly progressive necrotizing glomerulonephritis (RPGN) and, in some cases, lung hemorrhage (1).
In Korea, several case reports have been published on patients with MPA, but there have been no studies describing the clinical features and treatment outcomes of MPA in Korean patients. This retrospective study assessed the clinical manifestations and outcomes of MPA in Korean patients.
MATERIALS AND METHODS
We retrospectively reviewed the medical records of 18 patients diagnosed as having MPA at Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea, between 1989 and 2006. Diagnoses were based on the Chapel Hill consensus conference (CHCC) definition of MPA (1994) (2). In 13 of the 18 patients, MPA diagnosis was confirmed histologically by renal biopsy.
To classify MPA in Korean patients and compare results with those of other studies, we applied the inclusion criteria used in a large study of MPA (3), consisting of 1) presence of RPGN and/or alveolar hemorrhage; 2) histologic demonstration of small-sized vessel vasculitis or segmental pauci-immune necrotizing glomerulonephritis (GN); and/or 3) symptoms suggesting small-vessel involvement (e.g., purpura) without GN and/or alveolar hemorrhage.
Only patients with systemic vasculitis were included; patients with other small-vessel vasculitides, such as Wegener's granulomatosis, or other connective tissue disease-associated vasculitis, were excluded from this study. Antineutrophil cytoplasmic antibodies (ANCA) were not included as a criterion.
For each patient, the following data were recorded: gender, age, clinical features, laboratory and immunologic parameters at time of diagnosis, treatment, outcome, duration of follow-up, and cause of death. The clinical features included symptoms, signs and organ involvement at presentation and during follow-up. Laboratory parameters included white blood cell (WBC) and platelet counts, hemoglobin, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), creatinine, liver enzymes, and hematuria and proteinuria on urinalysis. Immunologic parameters included the presence of antinuclear antibody (ANA), ANCA, rheumatoid factor (RF), complement components C3 and C4, hepatitis B virus (HBV) surface antigen (HBsAg) and antibody (anti-HBs), HBV core antibody (anti-HBc), and anti-hepatitis C virus antibody (anti-HCV).
To evaluate the association between disease activity at time of diagnosis and outcome, we retrospectively applied the Five Factor Score (FFS) (4) and the Birmingham Vasculitis Activity Score (BVAS) (5) at the time of diagnosis. The FFS consists of proteinuria (>1 g/day), renal insufficiency (serum creatinine >1.58 mg/dL), severe gastrointestinal (GI) tract involvement (defined as bleeding, perforation, infarction, and/or pancreatitis), cardiomyopathy, and/or central nervous system (CNS) involvement, with the presence of each factor accorded 1 point. The BVAS is a clinical index of disease activity based on symptoms and signs in 9 separate organ systems; the maximum score is 63.
Treatment response was defined as the stabilization or attenuation of clinical symptoms, signs and laboratory abnormalities after initiation of treatment. Relapses were defined as new systemic manifestations of vasculitis or worsening of 1 or several of the initial manifestations of the disease.
Causes of death were classified into 3 subgroups: vasculitis-related, vasculitis-unrelated such as treatment side effects, and unknown.
Long-term survival of patients was determined by trying to contact patients or their first-degree relatives.
Kaplan-Meier life survival analysis and the log-rank test were used to assess patient survival and to compare survival relative to FFS, BVAS, age and presence of alveolar hemorrhage.
RESULTS
Clinical features
Of the 18 patients, 9 were men and 9 were women; their mean (±SD) age at the time of diagnosis was 62.4±12.7 yr (range, 22-83 yr), and the median duration of follow-up was 8 months (range, 0-108 months). Mean (±SD) time to diagnosis from the onset of symptoms was 1.9±2.4 months (range, 0.2-10 months). Clinical manifestations at the time of diagnosis and during the course of the disease are summarized in Table 1. Renal manifestations (n=18, 100%) and various general symptoms (n=18, 100%) were the most common features of MPA. Lung involvement was seen in 13 patients (72%). Other manifestations included peripheral neuropathy (n=7, 39%), skin rash (n=6, 33%), musculoskeletal pain (n=6, 33%), gastrointestinal involvement (n=5, 28%) and cardiac involvement (n=4, 22%).
Laboratory findings
At the time of admission, mean (±SD) WBC and platelet counts were 13.7±5.3×103/µL and 316±128×103/µL, respectively. Mean (±SD) levels of hemoglobin, ESR, CRP and creatinine were 8.6±1.8 g/dL, 71±40 mm/hr, 11.4±5.7 mg/dL, and 4.2±3.0 mg/dL, respectively.
At admission, 14 patients (77%) had renal insufficiency (creatinine >1.4 mg/dL), 16 (89%) had hematuria (>1+), and 11 (61%) had proteinuria (>1+). During the course of the disease, however, all patients had renal insufficiency (100%) and proteinuria (100%), and 17 patients (94%) had hematuria. Nine of 16 patients (56%) in whom 24 hr urine collection was performed had proteinuria >1 g per day, a component of the FFS.
ANCA were determined by enzyme linked immunosorbent assay (ELISA) in 17 of the 18 patients, and by an immunofluorescence (IF) assay alone in one patient. Myeloperoxidase (MPO)-ANCA was positive in 16 of the 17 patients in whom ELISA was performed, whereas proteinase-3 (PR-3)-ANCA was not detected in any patient (Table 2). In the one patient for whom immunofluorescence (IF) assay was performed, perinuclear ANCA was detected. Thus, ANCA were found to be present in 17 of the 18 patients (94%).
Other relatively common features at the time of diagnosis were presence of ANA (n=7, 38%), decreased level of C3 (n=6, 33%), and presence of rheumatoid factor (n=4, 22%).
Treatment, outcome and prognostic factors
Of the 18 patients, 17 (94%) were treated with a combination of steroids and cyclophosphamide. Cyclophosphamide was administered orally in 12 patients and intravenously in 5 patients. Of the 17 patients treated with steroids and cyclophosphamide, 11 (65%) showed stable disease or improvement. One patient with diffuse alveolar hemorrhage (DAH) who was treated with pulse steroid therapy plus plasmapheresis died within 10 days of the onset of DAH. All 7 patients with DAH were treated with additional plasmapheresis, but 5 (71%) showed aggravation of DAH independent of initial response to treatment. Overall, 11 of the 18 patients (61%) showed response to treatment.
Of the 18 patients, 9 (50%) underwent dialysis, but only one became dialysis-independent. Mean creatinine level decreased after treatment, with or without permanent dialysis (Table 3).
Ten of the 18 patients (56%) died, with 6 deaths related to vasculitis and 2 deaths related to infections such as pneumonia and sepsis. DAH (50%) was the most common cause of vasculitis-related death. We could not confirm the cause of death in 2 patients who were lost to follow-up (Table 4).
Five of the 18 patients (28%) relapsed during the follow-up period, with 3 patients showing new systemic manifestations of vasculitis and the other 2 exhibiting worsening of their initial manifestations. Organs involved at the time of relapse included the kidneys, CNS, GI, heart, and lungs. Median time to relapse was 1.4 months. Of the 5 patients who relapsed, 3 (60%) died.
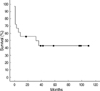
Overall mortality of MPA was 56%. Survival rates at 1 and 3 yr were 56% and 43%, respectively. Mean and median survival times were 53 months and 32 months, respectively (Fig. 1).
Mean FFS at the time of diagnosis was 1.44 (range, 0-2) and mean BVAS was 19.5 (range, 9-31). Survival curves according to FFS, BVAS, age and presence of DAH are shown in Fig. 2.
DISCUSSION
MPA was first recognized as a separate disease entity in 1948 in a subgroup of PAN patients with renal involvement characterized by segmental necrotizing GN (1). The clinical manifestations of MPA are very similar to those of PAN, but are characterized by the presence of RPGN and pulmonary capillaritis. In 1992, the term microscopic polyangiitis was adopted to connote a necrotizing vasculitis with few or no immune complexes affecting small vessels (capillaries, venules, and/or arterioles) (2), with MPA distinguished from PAN by the presence of small-vessel involvement. Because both MPA and Wegener's granulomatosis involve the small vessels, they share similar clinical features, such as DAH and GN; however, granulomatous inflammation is absent from MPA, differentiating it from Wegener's granulomatosis.
The overall clinical manifestations and disease courses in our patients were similar to those reported in other studies (Table 5). In contrast, while previous studies reported that MPA affects men slightly more often than women, we found a male:female ratio of 1:1. In addition, the mean age at the time of diagnosis in our patients was 63 yr, which is older than in previous reports.
Renal manifestations were the most predominant features of MPA in our patients. While renal insufficiency occurred in all patients during the course of disease, dialysis was required by only 50% of patients. In contrast, 25% to 45% of patients in previous studies required dialysis (6, 7).
DAH is the most serious form of lung involvement in MPA, reported in 12% to 29% of patients in several series (3, 6). We found, however, that pulmonary manifestations, especially DAH, were more frequent and severe in our patients. In contrast, involvement of the skin, GI tract and musculoskeletal system was less frequent in our patients than in previous reports, whereas cardiac manifestations, including pericardial effusion and cardiomyopathy, were more common.
Previous studies have reported that 50% to 80% of MPA patients are positive for ANCA (8-10). In one study, ANCA were present in 74.5% of patients at the time of diagnosis; among them, 87% had a perinuclear staining pattern (pANCA) and 13% had a cytoplasmic pattern (cANCA) (3). We found that 94% of our patients were positive for ANCA; of these, all had pANCA.
We found that 89% of our MPA patients also met the American College of Rheumatology (ACR) criteria for PAN (11), which include the presence of HBsAg or anti-HBs. Of our patients with MPA, 72% were positive for anti-HBs but none were positive for HBsAg. In Korea, 56% of PAN patients are positive for HBsAg or anti-HBs (12). HBV infection is endemic in Korea, with 5.1% of men and 4.1% of women in the 1998 Korean National Health and Nutrition Survey being positive for HBsAg (13). In addition, the prevalence of anti-HBs is high in Korea because of the global hepatitis B vaccination program. These findings suggest that using the presence of anti-HBs as a criterion for PAN would increase the false positive rate in the diagnosis of PAN in Korea. When we excluded individuals whose sole criterion for PAN was positivity for anti-HBs, we found that 50% of MPA patients satisfied the ACR criteria for PAN.
Combined therapy with high-dose steroids and cyclophosphamide has been indicated for patients with serious renal or pulmonary disease (14). Of our patients, only one was treated with steroids without cyclophosphamide, whereas 17 were treated with steroids and cyclophosphamide, making it difficult to compare treatment outcomes according to treatment regimen.
Mortality from systemic vasculitis has been shown to be significantly associated with disease severity, as assessed by the FFS and the BVAS (3, 4, 14). However, we did not observe significant relationships between mortality and these scoring systems. While disease-related mortality in our study was mainly associated with DAH, FFS does not reflect the latter.
The single most important prognostic factor in our study was DAH (p=0.0016) (Fig. 2D). This finding is consistent with previous reports showing that the relative risk of patient death was 8.65 times greater in patients with pulmonary hemorrhage (15).
To date, the efficacy of plasmapheresis in the treatment of MPA is unproven. Although all patients with DAH were treated with plasmapheresis in addition to steroids and/or cyclophosphamide, with 4 patients (57%) showing an initial response, 5 (71%) patients died during treatment. These findings suggest that the addition of plasmapheresis to combination treatment with steroids and cyclophosphamide for life-threatening DAH did not reduce mortality.
The overall mortality of our 18 patients with MPA was 56%, which was much higher than the 32.9% mortality rate previously reported (3). We also found that our MPA patients had a higher mortality rate than PAN patients in Korea (30%) (12). Higher mortality rate observed in this study may have been due to higher rate of DAH and the older age at onset. The latter is supported by the observation that the mean age at onset of non-survivors was higher than that of survivors (67 vs. 57 yr).
In conclusion, we have shown here that the clinical manifestations of MPA in Korean patients had several distinguishing features, including a higher rate of lung involvement, especially alveolar hemorrhage, which was the leading cause of death in our patients. We also found that cardiac manifestations were more frequent and musculoskeletal pain and GI involvements were less frequent in Korean MPA patients. Moreover, our MPA patients were older at disease onset and had a higher ANCA rate. Other overall clinical manifestations did not differ significantly.






 XML Download
XML Download