

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is the fifth most common malignancy in the world (1) and the third most common cause of death due to cancer in Korea (2). Multiple treatment modalities are available for patients with HCC, and hepatic resection has been successful as a treatment option with curative intent (3). However, more than 80% of patients are not candidates for surgical resection at the time of diagnosis due to advanced lesions and/or associated liver disease (4). In those cases, clinicians are confronted with the difficulty of selecting the optimal treatment option. The usual goals of the neoadjuvant therapy are to eradicate subclinical disease to reduce recurrence and the tumor bulk to prevent tumor spillage during operation. In the cases of large HCC greater than 5 cm in size, neoadjuvant treatments such as transarterial chemoembolization (TACE) and radiation therapy can be performed.
Initially, TACE was performed to treat unresectable HCC (5). Recently, TACE has been used as preoperative adjuvant therapy in patients with resectable HCC in the hope of increasing disease-free survival rates and improving long-term results after hepatectomy (6, 7). In those cases, however, the efficacy of improving postoperative survival remains controversial. Moreover, TACE alone frequently results in incomplete tumor necrosis (8).
Radiation therapy alone has been of limited benefit in the treatment of HCC. However, in several reports showing the results of HCC with combined treatment of radiation and chemotherapy, a beneficial effect has been suggested (9, 10).
Currently, surgical resection of advanced HCC following neoadjuvant treatment is challenging with the development of surgical techniques. Furthermore reductive or salvage surgery that resulted in the downstaging of unresectable HCC following palliative treatment showed some benefits for survival (11, 12). For large HCC, efforts to increase the curative rate and survival will be important in the search for various therapeutic modalities.
The efficacy of preoperative TACE and radiation therapy prior to hepatic resection has not been extensively reported. In this retrospective study, we analyzed sixteen patients with HCC greater than 5 cm in size that underwent hepatic resection after neoadjuvant combined TACE and radiation therapy.
MATERIALS AND METHODS
Between January 1994 and May 2007, 436 patients with HCC underwent hepatic resection. Among these patients, 16 patients with HCC of greater than 5 cm in size were given preoperative TACE and radiation therapy prior to hepatic resection at Severance Hospital, Yonsei University College of Medicine in Seoul, Korea. Medical records, histopathology, and survival data were reviewed and analyzed retrospectively.
TACE and radiation therapy were carried out as described below. TACE was performed with an infusion of a mixture of 5 mL iodized oil contrast medium (Lipiodol, Guerbet, Aulnay-sous-Bois, France) and 50 mg Adriamycin (Adriamycin, Ildong pharm, Seoul, Korea) and followed by embolization using gelatin sponge particles (Cutanplast, Mascia Bruneili Spa, Milano, Italy).
Patients that received radiation therapy in the primary lesion of the liver were included in the study, whereas patients who received radiation therapy in the extrahepatic metastatic organs were excluded. Simulating computed tomography (CT) scans were taken to determine the radiation volume for each patient, including the tumors with 2-3 cm margin.
We investigated the effect of preoperative TACE and radiation therapy through the reduction of the tumor size. We also evaluated the level of alpha-fetoprotein (AFP), Indocyanine Green retention rate at 15 min (ICG-R 15), Child-Pugh classification, operative factors, and pathologic results-tumor size and number, the presence of vessel invasion, the extent of tumor necrosis, and resection margin and stage according to the Japanese TNM classification (13).
The effectiveness of preoperative therapy on tumor response was evaluated by comparing serial CT scans before and after treatment. The response evaluation criteria in solid tumors (RECIST) (14) was used for evaluation of the tumor response. The RECIST uses unidimensional measurement. Complete disappearance of the tumor was considered as a complete response (CR). A reduction of at least 30% in the sum of the longest diameters of target lesions, taking as reference the baseline study, was considered a partial response (PR). An increase of at least 20% in the sum of the longest diameters of target lesions, taking as reference the smallest sum of the longest diameters recorded since treatment started or new lesions appeared, was regarded as a progressive disease (PD). However, neither the PR nor PD criteria were met, taking as reference the smallest sum of the longest diameters recorded since treatment started was regarded as a stable disease (SD). All patients received anatomical hepatic resections with the goal of achieving negative resection margins. In most patients, however, due to the cirrhosis and liver atrophy accompanied by huge liver mass, the achievement of enough resection margins being greater than 1 cm was difficult.
Patients were followed up at 1 month after operation and then every 3 months. Patients were screened for AFP, and they underwent dynamic CT. When intrahepatic recurrence was suspected, most of the patients underwent hepatic angiography or magnetic resonance imaging (MRI) to confirm the existence of recurrence.
Statistical calculations were performed using SPSS, version 13.0 for Windows (SPSS Inc. Chicago, IL, U.S.A.). Overall survival and recurrence rates were calculated using the Kaplan-Meier method.
RESULTS
The 16 patients examined in the study included 14 men and two women with a median age of 52.5 yr (ranging from 22-70 yr). The clinicopathological characteristics of the 16 patients are shown in Table 1. Fifteen patients had hepatitis B viral infection and 1 patient had hepatitis C viral infection. Median numbers of TACE performed preoperatively was three times and median radiation dosage was 45 Gy (with a range of 30-68 Gy). The median interval between the termination of radiation therapy and hepatic resection was 4.7 months. The median tumor diameter before the neoadjuvant therapy measured on the CT scans was 10.0 cm (with a range of 6.3-18.0 cm). Changes in tumor size comparing the CT scans before and after the treatment were following: size reduction was achieved in nine cases, an increase in tumor size was noted in three cases, and four cases displayed no change. None of the 16 patients demonstrated a CR, and only two patients showed a PR according to RECIST criteria. The response rate calculated for the proportion of CR and PR to 16 patients was 12.5% in preoperative CT scan.
All patients belonged to Child-Pugh class A before and after treatment.The median ICG-R 15 (preoperative status) was 12.7% (and ranged from 1.0-22.7%). Seven patients showed elevation of ICG-R 15 after treatment (ICG-R15 was not checked at initial diagnosis in three patients). The median value of AFP at initial diagnosis was 1,507.3 IU/mL (with a range from 4.4 to >50,000 IU/mL). The median value of AFP after treatment (just preoperative status) was 13.1 (with a range from 2.0 to 2,648 IU/mL). Thirteen patients demonstrated more than 50% decrease of AFP levels after treatment. Two patients demonstrated elevation of AFP levels after treatment.
Various surgical procedures were performed, including right hemihepatectomy (n=8), left hemihepatectomy (n=4), central bisectionectomy (n=1), trisegmentectomy (n=1) and bisegmentectomy (n=2). In the cases of large tumors combined with severe adhesion making difficulties in liver mobilization, anterior approach rather than conventional technique of liver mobilization was performed.
Thirteen of 16 patients had a single tumor. The median tumor diameter measured on the specimen was 9.0 cm (with a range of 5-18 cm). The degree of tumor necrosis noted upon microscopic examination was more than 80% necrosis in 15 patients. Microvessel invasion was detected in five patients. The pathology of the remaining liver was characterized as normal in three patients, as chronic hepatitis in eight patients, and as cirrhosis in five patients. Ten patients had pathological stage II tumors, four patients had stage III tumors, and two patients had stage IVA tumors accordingt to Japanese TNM system. Finally, the staging discrepancies were noted between the clinical and pathological stages in five patients whose tumor stages were upgraded due to microvessel invasion.
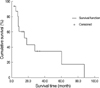
No postoperative mortality occurred in the cases reviewed in this study. The mean follow-up period was 24.2 months (with a range of 3.2-87.4 months) (Fig. 1). The median survival time was 13.3 months. The median disease-free survival time was 5.7 months. The patterns of recurrence were intrahepatic (n=7) and lung (n=2), and most recurrences occurred within 4 months of the operation. Eleven patients died due to tumor recurrences (n=8) and hepatic failure (n=2). Five patients survived more than 2 yr, and 2 patients survived more than 5 yr (Table 2). The two long-term survivors showed complete total necrosis of the tumor although 1 patient showed vascular invasion of the necrotic tumor. The pathology of remaining liver showed non-cirrhotic liver.
DISCUSSION
Several treatment modalities are available for patients with HCC, including TACE, radiofrequency ablation, hepatic arterial infusion, and radiation therapy. When adequate neoadjuvant treatment is achieved, sequential hepatic resection may be a valuable option for prolonging survival. However, the main problem with these tumor-shrinking treatments is that only a small proportion of patients respond well enough to allow hepatic resection following therapy, and the responders cannot be predicted.
The efficacy of salvage or reductive surgery for HCC following adjuvant therapy has been reported by several authors (11, 12, 15). Nevertheless, the efficacy of preoperative TACE is controversial. Some authors have demonstrated the adverse effects of preoperative TACE (16, 17), while others have reported its efficacy (7, 18). The main limitation of TACE is incomplete necrosis due to dual blood supply around the capsule, multiple collateral circulation, or recanalization of the embolized artery (19). Furthermore, patients with large HCC can rarely achieve complete remission by TACE alone.
To overcome the limitations associated with TACE, combined treatment with radiation therapy can produce synergistic effects such as the elimination of residual cancer cells following TACE. Tumor shrinkage after TACE allows the use of smaller irradiation fields, which permits higher tumor doses and improves normal liver tolerance. Furthermore, retainment of the anticancer drug in the tumor has been documented to have a radiosensitizing effect (20, 21).
There are few reports that have examined the patients with HCC who underwent hepatectomy following TACE and radiation therapy. The response rates of advanced and unresectable HCC treated with only TACE and radiation therapy were previously reported to be 18-65.8% in the review of the literatures (22-25). The response rate calculated by the proportion of CR and PR according to RECIST criteria based on CT scan was 12.5% (two of sixteen patients). However, actually the pathologic specimen showed CR in 10 patients (total necrosis) and PR in 5 patients (80-95% necrosis). Therefore reduction of tumor size in imaging study did not reflect the response to treatment exactly.
Fourteen patients showed greater than 90% necrosis. The role of tumor necrosis in patient prognosis remains controversial. Some authors reported that the extent of necrosis was not a favorable prognostic factor (26, 27). Other authors have reported that preoperative TACE resulted in better disease-free survival rates when complete tumor necrosis was induced (28). In our study, the two patients who survived beyond 5 yr showed total tumor necrosis on the specimen. In patients with partial necrosis, the remaining tumor cells are less firmly attached and more likely to be dislodged into the bloodstream during hepatic resection (28, 29). The residual viable cancer cells may facilitate tumor progression and induce intrahepatic metastasis. Such intrahepatic recurrences are considered to arise from intrahepatic metastasis by means of venous dissemination (30). However it is still unclear that tumor necrosis improves the disease-free survival or the pattern of recurrence after curative resection of HCC.
In the 16 patients who underwent hepatectomy following TACE and radiation therapy, tumors recurred in eight cases mostly within 4 months of the operation. The median survival duration was 13.3 months. The results from patients with unresectable or advanced HCC who were treated with TACE and radiation therapy for palliation and not given surgery at other institutions were reviewed due to rarity of hepatic resection after neoadjuvant TACE and radiation therapy. It seemed that the result of our study did not reveal any survival benefit when compared with the results of these studies (24, 31). In the previous study in our institute, the preoperative TACE and non-TACE group undergoing curative resection greater than 5 cm in size did not show significant difference in disease-free survival. And the 16 patients in current study did not reveal any disease free survival benefit comparing with these preoperative TACE and non-TACE group in our institute. And the pattern of recurrence between the TACE and non-TACE groups undergoing curative resection did not reveal any difference (27).
The efficacy of hepatectomy following TACE and radiation therapy was difficult to determine because the number of patients in this study was small. In this retrospective study, the prognosis of HCC patients who underwent hepatectomy following TACE and radiation therapy was not satisfactory although two long term survivors were noted. Surgical resection can be one of treatment option when the patient did not show complete response following TACE and radiation therapy. Therefore further research will be required to examine the survival and disease control effect in a prospective randomized study.


 XML Download
XML Download