

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Many complications occur during hematopoietic stem cell transplantation (HSCT) due to regimen-related toxicities and graft-related toxicities. The cytoreductive regimens that are used in conventional HSCT damage the rapidly dividing cell populations, particularly the bone marrow progenitor cells and mucosal epithelial cells. These deficits cause various bacterial infections during the neutropenic pre-engraftment period (1). In the pre-engraftment period, pulmonary edema syndromes can occur because of pulmonary infections, iatrogenic fluid overload, and cardiac dysfunction caused by prior treatments with anthracyclins or radiation (2). In addition to the pulmonary edema syndromes, hepatic veno-occlusive disease (VOD), acute graft versus host disease (GVHD), and engraftment syndrome (ES) are also common during the pre- and peri-engraftment period.
ES has both an obscure pathogenesis and disease definition. ES is characterized by a noninfectious fever and various other clinical findings during the early neutrophil recovery phase, including skin rash, pulmonary infiltrates, and weight gain (3-5).
We observed the characteristic clinical findings that mimic ES during the pre-engraftment period but not during the early neutrophil recovery period after HSCT. In this work, we describe these clinical findings as pre-engraftment syndrome (pES) and also report the results of a retrospective incidence and risk factor analysis for pES in pediatric patients who received HSCT from various stem cell sources.
MATERIALS AND METHODS
Patients
From September 1997 to March 2004 all patients who received HSCT with bone marrow (BM), peripheral blood (PB), and cord blood (CB) at Dong-A University Hospital were consecutively entered into this analysis, which was approved by the institutional review board of Dong-A University Hospital. Of the total 56 patients who received HSCTs during this period, 6 patients were excluded from the study because they did not have sufficient medical records. Sixteen patients had acute myelogenous leukemia (AML), 8 patients had acute lymphocytic leukemia (ALL), 5 patients had chronic myelogenous leukemia, 4 patients had myelodysplastic syndrome (MDS), 11 patients had severe aplastic anemia (SAA), 3 patients had neuroblastoma, 2 patients had Wiskott-Aldrich syndrome, and 1 patient had non-Hodgkin lymphoma (NHL). Sources for the hematopoietic stem cells (HSC) were bone marrow in 23 patients, peripheral blood in 13 patients, and cord blood in 14 patients (Table 1). The patients' median age was 8.4 yr (range: 1-18 yr) and the median weight was 33 kg (range: 6-76 kg). The male-to-female ratio was 1:0.61.
Conditioning regimens
All patients were treated with conventional doses of conditioning chemoradiotherapy. The conditioning regimens for allogeneic bone marrow transplantation (BMT) were busulfan/cyclophosfamide for leukemia (n=11) and MDS (n=4), cyclophosfamide/procarbazine/antithymocyte globulin (ATG) (n=6) or cyclophosfamide/thoraco-abdominal irradiation/ATG (n=2) for SAA. For the cord blood stem cell transplantation (CBSCT), the conditioning regimens were busulfan/melphaln/ATG for leukemia (n=10) and SAA (n=2) and busulfan/cyclophosfamide/ATG for Wiskott-Aldrich syndrome (n=2). For the autologous peripheral blood stem cell transplantation (PBSCT), the conditioning regimens were carmustine/etoposide/cytosine arabinoside/cyclophosfamide for AML (n=6) and NHL (n=1), busulfan/cyclophosfamide for ALL (n=2), and melphalan/etoposide/carboplatin for neuroblastoma (n=3). Finally, for the allogeneic haploidentical PBSCT, the conditioning was cyclophosfamide/procarbazine/ATG for the patient with SAA (n=1).
Supportive care
Hematopoietic growth factor support and isolation, as well as antibacterial, antifungal, and antiviral prophylaxis were performed according to institutional protocols. Briefly, all the patients received intravenous daily doses of granulocyte colony-stimulating factor (G-CSF, 5 µg/kg or 300 µg/m2) from day 0 or day 5 until an absolute neutrophil count (ANC) above 500/µL was achieved for 3 days. The patients also received packed red blood cell transfusions to maintain hemoglobin levels at 8.0 gm/dL or higher. Platelets were also transfused to keep the platelet count at 20,000/µL or greater. All blood products were irradiated to 1,500 cGy and then filtered prior to transfusion. In order to decontaminate the gut, all the patients received vancomycin plus kanamycin orally. Fluconazole was given for antifungal prophylaxis until an ANC above 500/µL was observed. Pnemocystis jiroveci prophylaxis consisted of trimethoprim/sulfamethoxazole until day-1. After this point, the treatment was resumed three times a week following the myeloid engraftment. Finally, all patients received prophylactic acyclovir and preemptive gancyclovir treatment for herpes simplex virus and cytomegalovirus infections.
Patients with fever had a comprehensive workup performed for infections that included urine culture and blood cultures through the peripheral line as well as through the central lines. This workup was followed by an empirical systemic antibiotic therapy.
Prophylaxis for GVHD
For GVHD prophylaxis, cyclosporin with or without methotrexate was used for allogeneic sibling BMT and methotrexate plus cyclosporin or tacrolimus was used for unrelated BMT. Cyclosporin with or without methylprednisone was used for CBSCT.
Definition of the pES
In order to characterize the pES, we used criteria similar to those that describe ES, but included only symptoms that occurred during the pre-engraftment period before neutrophil engraftment, not during the early neutrophil recovery phase. Engraftment was defined as absolute neutrophil count greater than 0.5×109/L for two consecutive days. Those symptoms are noninfectious fever and skin rashes mimicking GVHD with or without the evidence of fluid retention.
RESULTS
Incidence of pES
Seven out of 50 patients (14%) fulfilled the diagnostic criteria for pES. Of these seven patients, 4 were male and 3 were female. The median age and body weight of the patients with pES were 6.7 yr (1-12) and 25.7 kg (8-48), respectively. Three cases of pES developed in the patients who received unrelated CBSCT, 3 cases developed in the patients receiving allogeneic sibling BMT, and 1 case was observed in an unrelated BMT. pES did not develop in the patients who received PBSCT (Table 2).
Description of pES
The clinical characteristics of patients with pES are presented in Table 3. All 7 patients presented with noninfectious fever plus skin rashes with or without pulmonary infiltrates between day +5 and day +8. The fever duration for these patients was 3-7 days, and the time of onset for these symptoms was 4-15 days before neutrophil engraftment. Tachypnea with pulmonary infiltrates was recognized in 3 patients who received CBSCTs.
Four patients (UPN-3, 6, 12, and 18) who presented with fever plus skin rash without respiratory symptoms completely resolved with methylprednisone therapy. However, one of these patients (UPN-18) developed acute GVHD on day +20 and expired from complications due to multiorgan failure. One patient (UPN-35) who presented with fever plus skin rash with respiratory symptoms had a spontaneous resolution of the symptoms.
Another patient (UPN-36) developed fever plus skin rash with tachypnea on day +8 and abruptly progressed with worsening pulmonary edema and hypoxia. We treated this patient with methylprednisone and fluid restriction as well as endotracheal intubation. With these therapies, the pulmonary edema abruptly resolved on the next day (Fig. 1) and the neutrophils were engrafted on day +13. Finally, one patient (UPN-32) who developed fever plus skin rash with tachypnea on day +8 was treated with methylprednisone and fluid restriction. However, this patient expired on day +14 due to complications of pulmonary hemorrhage.
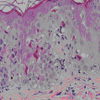
The histopathological findings of skin rashes in patients with pES (UPN-32) revealed similar findings compatible with those of acute GVHD (Fig. 2).
Risk factors and outcomes of the pES
We found no significant differences between the patients with and without pES occurrences with regard to gender, age, body weight, ABO incompatibility, human leukocyte antigen (HLA) disparity, infused cell dose, and the starting date of GCSF treatment. The source of stem cells, i.e., BM, PB, and CB, also had no impact on the pES occurrences (Table 4).
The engraftment speed was more rapid for patients with pES who received BMT (10.75±0.5, 10-11 day) than for patients without pES (12.31±2.47, 9-18 day) (p=0.032). Furthermore, the engraftment speed was also more rapid for patients with pES who received CBSCT (17.5±6.36, 13-22 day) than for patients without pES (32.14±15.12, 12-61) (p=0.143) (Table 5).
Acute GVHD appeared in 1 out of 7 patients (14.28%) who developed pES and in 4 out of 43 patients (9.30%) without pES. Hepatic VOD developed in 1 out of 7 patients (14.28%) with pES and in 2 out of 43 patients (4.65%) without pES. pES had no impact on the occurrence of acute GVHD (p=0.707) and hepatic VOD (p=0.342) (Table 5).
The 5-yr survival rate was 71.43% for patients with pES and 49.59% for patients without pES. However, we found no significant differences in the survival rate with regard to the occurrence of pES (p=0.417) (Fig. 3).
DISCUSSION
Many etiological factors can cause fever, skin rashes, and pulmonary infiltrates during the pre-engraftment period following HSCT. These factors include infections, chemotherapeutic or antibiotic agents, immunosuppressive agents, growth factors, and blood products (3, 4, 6). ES also contributes to the fever, skin rashes, and pulmonary infiltrates that develop in the early neutrophil recovery phase (3, 4). In this study, with the comprehensive septic workup and clinical course, we were able to show that concurrent infections, ES, and other etiologic factors are not the causative factors for fever, skin rashes, and pulmonary infiltrates. We considered the syndromes that presented to our patients before engraftment, were different from ES occurring during the early engraftment period. Therefore, the characteristic findings mimicking ES that were observed during the pre-engraftment period in this study could be another clinical syndrome that follows HSCT.
Takaue also observed this clinical syndrome in about 70% of CBSCT patients who received reduced-intensity conditioning regimens. He referred to this event as an "early inflammatory syndrome (EIS)" (personal communication, 2003). There have been no definite criteria or proven pathophysiological etiologies for this clinical syndrome until now. Thus, we preferred to describe this condition as "pre-engraftment syndrome" because it develops during the pre-engraftment period. Even though Takaue told that the incidence of EIS was about 70% in CBSCT patients, we observed pES in only 14% of all patients and in only 21.4% of the CBSCT patients. Further studies are required to determine whether the high incidence of EIS in Takaue's experience was related to the patient's characteristics or reduced-intensity conditioning regimens.
ES risk factors have been identified in many studies (7-10) and include gender (9), the infused cell dose (9, 10), the stem cell source (9), and G-CSF use (9). We also analyzed the risk factors for pES, but we could not find any with significance. However, these results might be related even with the small study size. Although other studies have reported that the ES occurred more frequently in autologous HSCT than in allogeneic HSCT (4, 5, 9), our study revealed that pES developed only in allogeneic HSCT, and not in autologous PBSCT.
The pathophysiology of ES has not been well clarified. The complex interplay of the microenvironment with the cytokines of the interacting cells, which occurs during the engraftment process, can play an important role in this syndrome (3, 10-14). These cytokines have been well correlated to neutrophil regeneration during the post-transplant period (10). Ravoet et al. (10) reported that neutrophil engraftment was more rapid and enhanced in patients with ES than in patients without ES. Although we did not perform these cytokine studies, we suspect that the positive impact of pES on the speed of neutrophil engraftment in this study may also be due to various cytokine effects.
In most patients, the pES was completely resolved either spontaneously or with methylprednisone and supportive therapy. The beneficial effects of steroid therapy may be derived from its immunosuppressive effect on cytokine reactions and from its anti-inflammatory nature. However, close observation is required for patients with pES because some cases became worse and were refractory to methylprednisone and supportive therapy.
In summary, we have described a new distinctive clinical syndrome that occurs during the pre-engraftment period. This syndrome is very similar with ES, yet unique in the timing of its occurrence. pES may be associated with enhanced engraftment and has no impact on the other clinical outcomes. However, patients with this syndrome should be closely monitored for the possibility of rapid deterioration and early therapeutic challenges. The disease entity and diagnostic criteria of pES are obscure; therefore, further multicenter clinical studies and pathophysiological research are required for better understanding of this newly described syndrome.







 XML Download
XML Download