

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transient mid- and basal ventricular ballooning is a new variant of transient left ventricular (LV) ballooning similar to transient LV apical ballooning syndrome, mainly due to emotional and physical stress (1-4). Its exact mechanism of pathogenesis remains unknown. We report transient mid- and basal ventricular ballooning associated with catecholamines in two patients. These cases showed similar clinical courses to transient LV apical ballooning syndrome and catecholamine-mediated myocardial dysfunction, which might be a potential mechanism of this syndrome.
CASE REPORT
Case 1
A 32-yr-old man presented to our emergency department with palpitation and squeezing chest pain. His initial blood pressure was 190/112 mmHg and electrocardiogram showed sinus tachycardia of 120/min. The initial electrocardiogram showed slight ST segment elevation in the inferior leads (lead II, III, and aVF). Echocardiography demonstrated a dilated mid portion of the LV and LV ejection fraction was 35% (Fig. 1A, B). However, the motion of the LV apex was normal. During the echocardiographic examination, his heart rate decreased suddenly to 70/min from 122/min. Serum level of creatinine kinase (CK) was 177 IU/L (normal range: 55-170 IU/L), CK-MB was 7.8 ng/mL (normal range: 0-4 ng/mL), and troponin I was 1.74 ng/mL (normal range: 0-0.05 ng/mL). The serum level of N-terminal-pro-B type natriuretic peptide (NT-pro-BNP) was increased up to 733 pg/mL (normal range: <200 pg/mL).
We performed emergent cardiac catheterization to rule out acute myocardial infarction. The coronary arteries were free of any organic stenosis and LV showed severe hypokinesia in the mid to basal portion. However, the LV apical wall motion was preserved (Fig. 2).
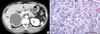
To rule out pheochromocytoma, we performed abdominal computerized tomography (CT). An abdominal CT showed an approximately 7.8×8.3×10.0 cm large septated cystic mass with irregular wall enhancement of the right adrenal gland (Fig. 3A). His serum catecholamine levels were reported as follows: epinephrine, 436.1 pg/mL (normal range: 0-140 pg/mL) and norepinephrine, 509.7 pg/mL (normal range: 0-450 pg/mL). The urinary catecholamine levels were as follows: epinephrine, 1,530.6 µg/day (normal range: 10-20 µg/day), norepinephrine, 1,048.8 µg/day (normal range: 15-80 µg/day) and metanephrine, 22,107.4 µg/day (normal range: 52-341 µg/day). From these findings, catecholamine induced cardiomyopathy showing midventricular ballooning was our final diagnosis.
The patient was treated with oral furosemide, an oral alpha blocker (prazosin) and intravenous nitrate infusion. The low dose of beta blocker was initiated after alpha blockade. The follow up echocardiography after three days of treatment showed marked improvement of LV systolic function and decreased LV dimension. The LV ejection fraction was 59%, with no regional wall motion abnormalities (Fig. 1C, D). He underwent successful surgical resection and the pathologic findings of the excised adrenal gland were compatible with pheochromocytoma (Fig. 3B).
Case 2
A 47-yr-old man with no cardiac history presented with hypotension after resection of an inverted papilloma of the left nasal cavity. He was treated with subcutaneous epinephrine (epinephrine HCl 1 mg/ample) injection, about 0.2-0.3 mL, to the nasal mucosa to prevent excessive bleeding. After the injection, his systolic blood pressure and heart rate transiently increased to 170 mmHg and 140/min, respectively, then decreased to 50 mmHg and 70/min, respectively. Electrocardiogram showed normal sinus rhythm and no significant change of his initial electrocardiogram.
Echocardiography demonstrated a dilated LV, akinesia of the basal to mid portion of the LV with sparing of apex and LV ejection fraction was 28% (Fig. 4A, B). Serum level of CK was 248 IU/L (normal range: 55-170 IU/L), CK-MB was 9.1 ng/mL (normal range: 0-4 ng/mL), and troponin I was 5.4 ng/mL (normal range: 0-0.05 ng/mL). The serum level of NT-pro-BNP was increased up to 4,277 pg/mL (normal range: <200 pg/mL). No coronary angiography was performed because of the low probability of coronary arterial disease and a normal preoperative treadmill exercise test. A follow-up echocardiogram obtained after two days of conservative treatment showed normalized LV size and function (Fig. 4C, D). The LV ejection fraction was 56%, with no regional wall motion abnormalities. Treatment with β-blocker and angiotensin converting enzyme inhibitor was initiated and continued for about one month after normalization of LV function.
DISCUSSION
We report two cases of transient mid- and basal ventricular ballooning syndrome associated with catecholamines. Transient mid- and basal ventricular ballooning is a new variant of the transient LV apical ballooning syndrome, which is also known as "stress cardiomyopathy", and includes transient cardiac contractile abnormalities and heart failure precipitated by acute emotional or physical stress. However, the involvement of the LV's mid- and basal ventricle with sparing of the apical segment is the unique finding of this variant (1, 2). Proposed potential mechanisms of transient LV apical ballooning are multivessel epicardial spasm, microvascular dysfunction of the coronary arteries, impaired fatty acid metabolism, myocarditis and catecholamine-mediated myocardial dysfunction (1, 3, 5). Although the mechanism underlying the association between sympathetic stimulation and myocardial stunning is unknown, several proposed mechanisms have been proposed including coronary arterial spasm (6) and direct injury to myocytes (7). Moreover, transient LV apical ballooning can be observed in patients with excessive circulating catecholamines with pheochromocytoma (8). Although there was a case report of apical ballooning associated with pheochromocytoma, our report seems to be the first to demonstrate that mid- and basal ventricular ballooning is related with high blood catecholamines (8).
The reason for apical ballooning with sparing of the basal segment is unknown. One possible explanation is different distribution of sympathetic nerves (9) and dissimilar density of sympathetic nerves in the heart (10), which make the apex more vulnerable to a sudden increase in circulating catecholamine levels. In our cases, the patients showed severe mid- and basal ventricular dysfunction from transient elevation of blood catecholamine level probably due to hemorrhagic necrosis of the adrenal pheochromocytoma and injection of epinephrine, respectively. The variations in segmental involvement regardless of coronary anatomy in patients with excessive catecholamine levels may suggest different susceptibility to sympathetic stimulation from individual to individual.



 XML Download
XML Download