

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multiple myeloma (MM) is a neoplasm of plasma cells and is responsible for about 1% of all malignant neoplasms and about 13% of hematologic malignancies (1). The most common immunologic subtype of MM is immunoglobulin (Ig) G, followed by IgA and light-chain only. In comparison, IgD MM, which was first recognized by Rowe and Fahey (2), affects less than 2% of all patient with MM (3). It is known to have a more aggressive clinical behavior than other subtypes of MM and is associated with relatively high frequencies of renal failure, extramedullary involvement, hypercalcemia, amyloidosis, and Bence-Jones proteinuria, as well as a short survival period (4-7).
When compared with standard-dose chemotherapy for MM, high-dose chemotherapy in combination with autologous stem cell transplantation (ASCT) has been shown to significantly improve rates of complete remission (CR), CR duration, event-free survival (EFS), and overall survival (OS) (8-10). Recently, it was shown that outcomes of ASCT are superior to those of standard-dose chemotherapy in a series of 25 patients with IgD MM (11). However, few studies have compared the response to ASCT of patients with different MM subtypes (12, 13).
We have retrospectively analyzed 77 patients with MM who underwent ASCT in our center. The aim of our analysis was to evaluate EFS and OS after ASCT in patients with different MM subtypes.
MATERIALS AND METHODS
Patients
Between November 1998 and January 2005, a total of 77 patients with MM were treated with ASCT at the Asan Medical Center. All patients had adequate stem cell collection and met all the eligibility criteria of the ASCT protocol including age ≤70 yr and adequate cardiopulmonary and hepatic functions. At study entry, the exclusion criterion was poor performance status, as shown by an Eastern Cooperative Oncology Group (ECOG) score ≥3. All patients gave informed consent.
The study population was divided into two groups based on MM subtype: patients with IgD MM (8 patients); and those with other MM subtypes (69 patients).
Prior to ASCT, patients had received one to two lines of treatment, while 88% of the cases had received only one regimen of chemotherapy. Most patients were treated with VAD (vincristine, adriamycin, and dexamethasone) (67 patients, 87%) or VAD like regimen (6 patients, 8%), while four patients (5%) had received MP (melphalan, prednisone) as first-line treatment. At the time of transplant, 22% of patients were in CR. The vast majority had achieved a partial response (PR) with previous chemotherapy regimens, while 7 (9%) of them had stable disease. The median time interval between diagnosis and transplant was 5.6 months (range: 1.8-83.5 months). Of the patients, 13 (16.9%) had a second transplant; 4 of these had a planned second ASCT in CR and 9 were autografted after relapse or progression of their disease.
Treatment protocol
Peripheral blood stem cells were collected during 1-3 consecutive leukaphereses, following high-dose cyclophosphamide 4 g/m2, i.v., with subsequent lenograstim at 10 µg/kg/day from day 3 to the last day of leukapheresis. The concenturation of circulating peripheral blood hematopoietic progenitor cells (HPCs) were monitored daily, and when HPCs become 5 cells/µL, autologous stem cell harvest was performed (14). Peripheral blood stem cell were harvested with a target concentration of 10.0×106 CD34+ cells/kg.
High-dose chemotherapy was performed 3 and 2 days before stem cells infusion (day -3 and day -2). High-dose chemotherapy comprised melphalan 100 mg/m2 iv infusion for 30 min on each of theses two consecutive days (total 200 mg/m2). Stem cells were infused on day 0. Subcutaneous lenograstim treatment 5 µg/kg/day was started on day 1 and continued until the absolute neutrophil count was measured as ≥1,000 cells/µL on two consecutive days. The second ASCT was performed within 3-9 months of the first ASCT in all patients who had second ASCT except one, for whom the interval was 4 yr. The second ASCT was performed following the same procedure as the first ASCT.
Staging and response criteria
At the time of ASCT, staging was performed according to the Southwest Oncology Group (SWOG) staging system (15) and the 2005 International Staging Sytem (ISS) guidelines (16). The European Group for Blood and Marrow Transplant (EMBT) criteria were modified for assessing disease response (17). CR was defined as absence of monoclonal Ig from the serum and/or urine as shown by immuno-fixation analysis and less than 5% plasma cells on bone marrow aspirate (and biopsies, if performed). Patients were considered to be in PR if there was at least a 50% reduction in the serum M-protein concentration and a reduction in the level of Bence-Jones proteinuria by greater than 75% reduction or to less than 0.2 g/24 hr. No change was defined as no change or a reduction in paraprotein levels of less than 50%. Progressive disease (PD) was defined as a confirmed >25% increase in the serum paraprotein concentration compared with the level at the time of the best response, an increase in Bence-Jones proteinuria to more than 1.0 g/24 hr, or other unequivocal signs of disease progression, such as hypercalcemia, progressive skeletal disease, or soft tissue plasmacytoma. Relapse was defined as the reappearance of paraprotein in the serum of patients who achieved CR and an increase of greater than 25% in the serum paraprotein concentration, or other unequivocal signs of disease progression such as hypercalcemia or the development of new extramedullary disease for patients who did not achieve CR. Patients were considered to be in continued CR or continued PR if the CR/PR status attained after the induction chemotherapy was continued after ASCT.
Evaluation and follow-up
Patient responses were first evaluated 4 weeks after ASCT. Protein electrophoresis and immuno-fixation analyses of serum and/or urine were performed. If CR was achieved, the patient was evaluated every month for the first 2 months, then three times at 2 month intervals, and every three months thereafter. If CR was not achieved initially, the patient was evaluated every month until CR was achieved. At each follow-up visit, the patient's clinical history was recorded and he or she underwent a physical examination, complete blood count, platelet count, and liver function tests, and serum and/or urine protein electrophoresis analyses. If relapse or progression was confirmed, the decision of whether to perform further therapy was at the discretion of the participating physicians.
Statistical analysis
The proportions of patients with a given characteristic were compared with the use of χ2 test or Fisher's exact test. Differences in continuous variables were analyzed with the Student's t-test and confirmed with the use of the Mann-Whitney U test. All tests were two-tailed. An event was defined as progression, relapse, or death due to any cause. EFS was calculated for all patients from the date of ASCT. OS was calculated from the date of ASCT to death of the patient or to the date the patient was last known to be alive. Kaplan-Meier curves for EFS and OS were plotted and compared using the log-rank test. Prognostic factors for survival were determined by means of the Cox proportional-hazards model for multivariate analysis, which was performed for significant univariate variables. A p value <0.05 was considered significant. All calculations were performed using SPSS version 12.0 for Windows (SPSS Inc., Chicago, IL, U.S.A.).
RESULTS
Patient characteristics
A total of 8 patients with IgD MM were identified, accounting for about 10% of the study population. In this study, 36 patients (47%) had IgG MM, 17 patients (22%) had Ig A MM, and 16 patients (21%) had free light-chain MM.
Table 1 shows the base-line characteristics of the 77 patients. The median age of the patients was 51.0 yr (range, 20-68 yr). There were no significant differences in patient characteristics at baseline between the two groups (those with IgD MM vs. those with other MM subtypes). The two groups were specially similar in lines of prior chemotherapy, interval from diagnosis to ASCT, disease status prior to ASCT, and the proportion of patients who had second ASCT, which could have influence on outcomes following ASCT. Forty patients were checked for cytogenetic abnormalities, of whom 24 patients (60%) showed abnormalities. Nine patients had chromosome 13 deletion or hypodiploidy both of which are known to be poor prognostic factors (18).
Treatment-related toxicity
The treatment-related mortality (TRM) was 3% (2/69 patients) in the group of patient with other MM subtypes. The cause of death was septicemia. There was no treatment-related mortality in the IgD MM group. No patient developed grade III-IV cardiac, pulmonary, renal or liver toxicity (World Health Organization scale), whereas neutropenic fever was present in almost all patients and severe mucositis was observed in a third of the patients.
Response rate
Table 2 shows the patient responses to ASCT. The overall response rate (CR and PR) was 96%. Specifically, the CR rate was 75% for patients with IgD MM, compared with 58% for patients with other MM subtypes (p=0.81). In the IgD MM group, 5 patients (63%) were in continued CR/PR. In the group of patient with other MM subtypes, 37 patients (54%) were in continued CR/PR.
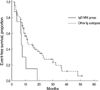
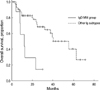
EFS and OS after ASCT
In this study population, the median follow-up was 17.2 months and the median OS was 39.3 months. In the IgD MM group, the median follow-up was 17.1 months (range, 4.7 to 29.7) from the time of ASCT. The median EFS and OS were 6.9 and 12.0 months, respectively. Of the 6 deaths in this group, all were attributed to MM. In the group of patient with other MM subtypes, the median follow-up was 17.2 months (range, 1.1 to 71.3) from the time of ASCT. The median EFS and OS were 11.5 and 55.5 months, respectively. Of the 21 deaths in this group, 13 were attributed to MM, 7 to infection, and 1 to suicide. Patients in the IgD MM group had significantly shorter EFS (p=0.01) (Fig. 1) and OS (p<0.01) (Fig. 2) compared with patients with other MM subtypes. There were no significant differences in OS and EFS among patients with other MM subtypes (p=0.7 and p=0.9, respectively). The median OS in other MM subtypes was 62.6, 40.0, and 55.5 months, and the EFS was 10.6, 11.2, and 15.0 months for IgG, IgA, and free light chain subtype, respectively.
In patients with chromosome 13 deletion or hypodiploidy, the median OS was 39.3 months.
Factors associated with EFS and OS following ASCT
In this study population, age, performance status, lines of prior chemotherapy, interval from diagnosis to ASCT, hemoglobin, creatinine, and albumin levels at the time of ASCT, and response after ASCT showed no association with either EFS or OS. However, the level of β2-microglobulin at the time of ASCT was significantly associated with EFS and OS.
OS after ASCT was associated with the SWOG stage at the time of ASCT. The median OS was 62.6 months in patients with SWOG stage 1, 24.5 months in patients with SWOG stage 2, and 31.9 months in patients with SWOG stage 3. In this study, patients with SWOG stage 1 had longer EFS and OS compared with patients with SWOG stage 2 or greater (p=0.173 and p=0.011, respectively).
The median OS was 62.6 months in patients with ISS stage 1, 37.8 months in patients with ISS stage 2, and 23.1 months in patients with ISS stage 3. Differences in EFS and OS among patients with different ISS clinical stages at the time of ASCT were not statistically significant (p=0.78 and p=0.185, respectively).
The results of univariate analysis are summarized in Table 3. Statistically significant prognostic factors for OS in the univariate analyses were SWOG stage 1, IgD subtype, and β2-microglobulin, whereas the prognostic factors for EFS were only IgD subtype and β2-microglobulin. The results of multivariate analyses are presented in Table 4. Based on the results of multivariate analyses, the prognostic factors associated with significantly shorter OS were IgD subtype (p= 0.002) and SWOG stage 2 or greater at the time of ASCT (p=0.01), whereas the prognostic factor associated with shorter EFS was only IgD subtype (p=0.023).
DISCUSSION
We found that patients with IgD MM had significantly shorter survival after ASCT compared with patients with other MM subtypes (relative risk: 4.6; p=0.002). However, the initial response to high dose chemotherapy and ASCT was similar in patients with IgD MM and patients with other MM subtypes. The overall response rate (CR and PR) following ASCT was 100% in the IgD MM group and 97% in patients with other MM subtypes, similar to that reported from other studies (9, 12, 13, 19). However, patients with IgD MM experienced earlier relapse/progression. The cumulative incidence of relapse/progression at 1 yr was 85% in patients with IgD MM and 51% in patients with other MM subtypes (p=0.009). These results are in agreement with those of previous studies comparing responses to conventional chemotherapy and survival rates in patients with IgD MM and patients with other MM subtypes (3, 4, 6, 7).
Only 1-2% of all MM cases are of the IgD subtype (3). In the present patient group, however, the frequency of IgD MM was about 10%. Due to patients' preference for our hospital and referral bias, the spectrum of MM patients treated at the Asan Medical Center was likely to be biased.
The Durie-Salmon clinical stage at the time of ASCT does not correlate well with prognosis (20), whereas the ISS stage or SWOG stage at the time of ASCT do correlate well with prognosis (15, 16). In addition, increased β2-microglobulin and reduced albumin levels immediately prior to ASCT are known to be adverse prognostic factors (13, 19-21). In our study, IgD subtype and SWOG stage at the time of ASCT were found to be independently associated with OS after ASCT. Although both the ISS and SWOG stage are based on β2-microglobulin and albumin levels, in this study the SWOG stage seemed to be more useful for predicting prognosis. Our study was not able to confirm the prognostic use of cytogenetics because this information was only available for 40 patients (52%).
Most investigators consider IgD MM to be a particularly aggressive subtype of MM, which affects younger patients, has a high frequency of extramedullary involvement, and is associated with renal function impairment, amyloidosis, and a short survival period. However, few studies have compared survival after ASCT for patients with MM of different subtypes, and their results are inconsistent. Terpos et al. reported that patients with non-secretory MM tend to experience better outcomes than those with secretory MM (13), and Sirohi et al. reported that patients with light chain MM had a significantly shorter OS than did patients with IgG or IgA MM (12). In those studies, however, only one patient had IgD MM. In the present study, we found no significant differences in OS and EFS among patients with other (non-IgD) MM subtypes (p=0.7 and p=0.9, respectively).
IgD subtype is associated with poor prognosis, so patients with IgD MM need to be treated more aggressively. Advanced stage IgD MM, according to SWOG or ISS staging systems, could be treated with tandem ASCT, maintenance therapy with thalidomide after ASCT or allogeneic stem cell transplantation (22-25).
This study had several potential limitations. First, this was a retrospective study from a single center. Second, the two groups were not matched due to the small number of patients (especially IgD subtype). However, two groups were similar in baseline characteristics. Despite these limitations, this is the first report showing poor clinical outcomes after ASCT for patients with IgD MM in Korea.
In conclusion, the response to ASCT of patients with IgD MM is similar to that of patients with other MM subtypes. However, patients with IgD MM have poor survival rates after ASCT compared with patients with other MM subtypes.




 XML Download
XML Download