

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It has been reported that the incidence of thyroid nodule in Graves' disease patients varies from 10% to 35% (1-9). It is possible that high-resolution ultrasonography during initial diagnosis allowed identification of small thyroid nodules in Graves' disease patients. However, the prevalence of differentiated thyroid cancer (DTC) in Graves' disease patients remains as a matter of debate, with previous reports showing the prevalence was 0.3-16.6% (1-14).
The biologic behaviors and optimal management of DTC with concurrent Graves' disease are still controversial. Some investigators have reported that patients of DTC associated with Graves' disease experienced a more aggressive course than euthyroid patients (15, 16). Pellegriti et al. (17) suggested that the extent of surgery in such patients must be extensive, involving at least a total thyroidectomy and lymph node dissection followed by 131radioactive iodine therapy (RI). In contrast, others reported that the aggressiveness and the treatment outcomes of DTC in Graves' disease patients are similar to those of euthyroid patients (6, 18). Thus, there remains controversy as to the optimal extent of surgery in these cases.
The aims of the present study were to identify clinicopathologic features, treatment outcome, and indicators for predicting locoregional recurrences and to suggest the optimal extent of surgery in DTC patients with concurrent Graves' disease.
MATERIALS AND METHODS
Study patients
During the 20-yr period from 1986 to 2005, 779 patients with Graves' disease underwent surgery at our hospital. The diagnosis of Graves' disease was based on the history and signs of thyrotoxicosis, increased levels of serum triiodothyronine (T3) and thyroxine (T4), low levels of thyroid-stimulating hormone (TSH), the presence of autoantibodies (thyroid stimulating antibodies [TSAbs] and/or antiperoxidase antibodies), increased radionuclide uptake at scintiscan, and the histological features of diffuse hyperplasia of the thyroid gland. Patients were treated preoperatively with propylthiouracil, cabimazole, or methimazole. They also received Lugol solution (8 drops per 6 hr) for 7 to 10 days before surgery. The indications for surgery were the presence of a large compressive goiter, recurrent thyrotoxicosis, side effects of antithyroid medications, unlikelihood or inability of taking medicine, presence of cold nodules on thyroid scanning, and suspicion of malignancy on fine needle aspiration biopsy.
Diagnostic timing
Study patients were classified as clinically overt carcinoma or incidental carcinoma. In clinically overt carcinoma, a patient with Graves' disease was found to have a specific symptom or sign and thyroid carcinoma was diagnosed preoperatively. However, in incidental carcinoma, Graves' disease was the only clinical diagnosis before operation and thyroid carcinoma was identified during surgery or following histological examination of permanent sections.
Surgical method
Patients with incidental carcinoma underwent a bilateral subtotal thyroidectomy or a Hartley-Dunhill operation (16) (a unilateral lobectomy with a contralateral subtotal lobectomy, leaving 4-6 g of thyroid tissue). Intraoperative frozen sections were carried out in all the suspicious lesions. In case of clinical carcinoma, we performed the operative methods according to the TNM classification system (T, tumor size; N, involvement of lymph nodes; M, presence of distant metastasis) (19).
Postoperative follow-up
All patients were postoperatively followed up every 3-6 months. Patients were evaluated for locoregional or distant metastasis by the following diagnostic methods: serum thyroglobulin/anti-thyroglobulin antibody level, ultrasonography, computed tomography, radioiodine scintigraphy.
RESULTS
Clinical characteristics
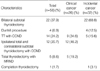
Fifty-eight cases of DTC (7.4%) were diagnosed among 779 Graves' disease patients who underwent thyroidectomy between 1986 and 2005. The study enrolled 8 male and 50 female patients with a mean age of 40.8±12.7 yr (range, 15-70). No patients had previous history of radiation exposure or radioactive iodine therapy. Twenty-six cases of clinically overt thyroid carcinomas were diagnosed among 779 Graves' disease patients (3.3%). The prevalence of incidental carcinoma in the Graves' disease patients was calculated as 4.2% (32 patients with occult thyroid carcinoma out of 753 patients who underwent operation represented only part of Graves' disease). Comparison of clinical findings of incidental and clinical carcinoma patients revealed no difference between the two groups in terms of duration of thyrotoxic symptoms, T3/T4 serum levels before the administration of antithyroid medication, and postoperative 6-week serum concentration of thyroglobulin/TSH (Table 1).
Surgical treatment and histopathologic findings
Of the 26 patients with clinical carcinoma, 14 underwent total thyroidectomy and 12 underwent subtotal thyroidectomy. Of the 32 patients with incidental carcinoma, 5 underwent total thyroidectomy and 26 subtotal thyroidectomy (Table 2). There was one patient of completion thyroidectomy, who had initially underwent a subtotal thyroidectomy for Graves' disease; the subsequent histopathology analysis, however, showed a widely invasive follicular carcinoma. Of the total 58 carcinomas, 57 (98.3%) were papillary thyroid carcinoma and 1 (1.7%) was a follicular thyroid carcinoma. The mean tumor size was 13±9 mm in diameter (range, 3-62). Extracapsular invasion and invasion to adjacent structure were found in 23 (39.7%) and 3 cases (5.2%), respectively. Multiple lesions were noted in 18 cases (31.0%). Central compartment node metastasis and lateral cervical lymph node metastasis were shown in 18 (31.0%) and 5 (8.6%) cases, respectively.
Postoperative adjuvant therapy
Sixteen patients treated with total thyroidectomy underwent postoperative adjuvant RI. Eleven of these patients received low-dose (30-60 mCi) therapy for ablation of residual thyroid tissue. Four patients in which lateral cervical lymph node metastasis was present received high-dose (150-250 mCi) therapy.
Treatment outcome and Indicators for predicting recurrence
The mean follow-up period was 116.8±54.0 months (range, 23-260). For all the patients, the 10-yr overall survival and disease-free survival rates were calculated to be 95.8% and 91.1%, respectively (Fig. 1). Local recurrence was identified in 4 patients (6.9%), all of whom belonged to the clinical carcinoma group. The mean duration of recurrence was 129±36 months (range, 91-167), with no patients diagnosed with distant metastases during the follow-up.
Of the 4 loco-regional recurrence patients, 2 patients underwent re-operation and high-dose RI. Neither of these patients has shown any evidence of recurrence up to now (77 months and 54 months, respectively) since the second operation. For the other 2 patients, local recurrence was noted in the thyroid bed and lateral cervical lymph nodes, respectively (Table 3). These patients were not treated for this local recurrence since both refused to undergo treatment: one died of aggressiveness of local recurrence 132 months after the initial thyroidectomy and the other of combined ovary cancer with systemic metastasis 98 months after the surgery.
The patient age of over 45 yr, tumor size, multiplicity, extracapsular invasion, and clinical cancer were significant factors in predicting the locoregional recurrence (Table 4).
DISCUSSION
The prevalence of thyroid carcinoma in Graves' disease has been reported to be from 0.3% to 16.6% (1-14). It is suggested that part of the explanation for the wide variation in incidence could be due to differences in the extent of resection as well as in the number of histologic sections examined per specimen (20). Moreover, the increasing use of high resolution ultrasonography has revealed greater numbers of thyroid nodules, and the routine use of such devices has allowed diagnosis of small thyroid carcinoma in Graves' disease patients. The 7.4% prevalence found in our work seems to be relevant to that found in other reports.
Controversy remains regarding the pathogenic relationship between thyroid carcinoma and Graves' disease. It is well known that the binding of TSH to TSH receptors might promote the growth of cancer cells in euthyroid patients with thyroid carcinoma. In Graves' disease in which serum TSH is suppressed, TSAbs rather than TSH are reported to activate the TSH receptor (16, 21, 22). Some studies showed that autoimmune responses in Graves' disease including TSAbs are closely linked to angiogenesis, which plays a crucial role in tumor growth and development (15, 21, 23). Therefore, patients of Graves' disease with DTC has been found to have a worse clinical outcome than euthyroid patients with DTC (4, 17, 18, 24, 25). In contrast, other investigators suggested that Graves' disease was not related to the aggressiveness of coexisting thyroid carcinoma (6, 9, 26). These studies identified that the severity of thyrotoxicosis was not related to the prognosis of DTC patients with concurrent Graves' disease (27-29). In the present series of our work, the 10-yr overall and disease-free survival rates were 95.8% and 91.1%, respectively, showing favorable treatment outcomes in these patients, and the severity of thyrotoxicosis and serum thyroid hormone levels did not affect the prognosis.
A few studies examined recurrence-predicting indicators in patients of DTC with concurrent Graves' disease. Although some authors suggested patient age, tumor size and preoperative T3 levels are significant factors to predict metastasis (6, 30), recent studies indicate that the most crucial prognostic indicator is diagnostic timing (clinical or incidental) (26, 31). In the present investigation, patient age over 45 yr, the presence of extracapsular invasion, multiplicity, and clinical cancer, but not severity of thyrotoxicosis, were correlated with a high recurrence rate.
Debate continues regarding the proper extent of surgery for Graves' disease patients with DTC. There has been a preference for radical surgery in patients with DTC with concurrent Graves' disease, involving at least total thyroidectomy and lymph node dissection followed by RI (16, 17). However, recent approaches have suggested that the choice of surgical strategies depend on the diagnostic timing and stage of tumor (26-31). This indicates that the extent of surgery should be similar for thyroid cancer in euthyroid patients, and that subtotal thyroidectomy is sufficient, whereas additional completion total thyroidectomy is not necessary in incidental cases. In the present investigation, neither the extent of thyroidectomy nor the presence of lymph node dissection was found to be correlated with the recurrence rate. Therefore, complete thyroidectomy might be helpful only in cases in which indicators predicting recurrence are present. In this study, two of the four patients who had local recurrence underwent second operation and survived with no further episodes. The other two patients refused further treatment and died. Even though the present study involved only a small number of patients, the findings suggest that early detection and active treatment lead to a good prognosis even in cases of local recurrence.
Nevertheless, we encountered with several limitations when we tried to investigate the treatment outcome and significant factors to predict recurrence in thyroid carcinoma patients with concurrent Graves' disease. First, there were only a limited number of patients. Second, the natural course of DTC is characterized by very slow progression, therefore, our observation period might not have been enough to detect the evolution from silent disease to overt clinical metastasis.
In conclusion, we recommend that patients of Graves' disease should undergo regular screening both meticulous physical examination and ultrasonography for early detection of thyroid carcinoma. Our present results show that predicting factors for recurrence in DTC patients with concurrent Graves' disease were age over 45 yr, tumor size over 10 mm, multiplicity, extracapsular invasion, and clinical carcinoma. We also suggest that the choice of extent of surgery in these patients should depend on the diagnostic timing (clinical or incidental) and factors for predicting recurrences, and that a subtotal thyroidectomy would be sufficient in incidental carcinomas without factors predicting recurrence. On the other hand, in clinical cancers or in cases where recurrence-predicting factors are present, at least a total thyroidectomy with lymph node dissection might be helpful.




 XML Download
XML Download