

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Severe limbal epithelial cell deficiency, that occurs with the Steven-Johnson syndrome (SJS) or thermal and chemical burns, often causes covering of the corneal surface by invading neighboring conjunctival epithelial cells with ingrowth of fibrotic tissue, stromal scarring, and neovascularization (1). Because of these injuries, there is significant epithelial cell damage, and the prognosis after penetrating keratoplasty is usually poor. Therefore, alternative surgical treatments such as keratoepithelioplasty and limbal transplantation have been developed to improve the outcome of ocular surface reconstruction of the severely injured eye (2-5). Recently, attention has been focused on the use of ex vivo cultivated corneal epithelial cell transplantation; this is a new approach to ocular surface reconstruction for severe ocular surface disease (OSD) (6-8). However, there are many problems with this approach such as inflammation, infection, prolonged use of immunosuppressant therapy in the allograft, neovascularization, the development of epithelial opacities, and subepithelial opacities in the cultivated oral mucosal epithelial transplantation. Furthermore, extra time, equipment and facilities for culture are necessary, and continuous management and special technology are needed during the culturing process. Therefore, we attempted to overcome the problems associated with ex vivo allogenic transplantation by using in vivo expansion. Previously, we reported ultrastructural analysis of in vivo expanded corneal epithelium on amniotic membrane (AM) in damaged cornea. We found that at least 3 months might be needed for the differentiation and proliferation of cells prior to transplant (9).
In this study, in vivo expansion of corneal epithelium in healthy cornea was performed; after adequate growth, the epithelial sheet was transplanted into a severely damaged cornea. We reported three cases with a persistent epithelial defect (PED) with limbal stem cell deficiency were successfully managed with surface reconstruction.
MATERIALS AND METHODS
Patients
Three patients with intractable PED were chosen for transplantation. The intractable PED was diagnosed after five months of standard medical and surgical treatment; preservative-free artificial tear, serum therapy, epidermal growth factor (EGF) solution, therapeutic contact lens, and amniotic membrane transplantation - temporary and permanent. These patients had nearly total limbal deficiency in both eyes due to several diseases. A blood type-matched living related donor underwent epithelial peeling, followed by denuded amniotic membrane transplantation (AMT) in the nondominant eye; then the corneal epithelial cells were expanded in vivo. Informed consent for the surgical procedure was obtained from each patient and their participating relatives. We performed in vivo cultivated corneal epithelial transplatation in three eyes in three patients with severe ocular surface disease: the primary diagnosis was a chemical burn in two cases and SJS in one (Table 1). The eyes received cultivated corneal epithelial transplantation for the purpose of covering the corneal surface and avoiding the complications that accompany PED.
Amniotic membrane
AM was prepared at Bioland Korea (Cheonan, Korea) with following method. After informed consent, human AM was obtained at the time of cesarean section delivery. Under sterile conditions, the AM was washed 3 times in 1,000 mL of normal saline containing antibiotics (80 mL of Gentamicin sulfate), and all blood clots were removed. The AMs were frozen in preservative solution (Dulbecco's modified eagle's medium [DMEM] and glycerol mixed solution) and stored at -70℃; they were thawed just before use.
Preparation of the in vivo grown epithelial sheet using AM
The amnion cells were removed by gentle scrubbing with a 20% alcohol soaked scraper. The AM was trephinized into 8 mm-diameter round excisions. First, the epithelial cell layer of the healthy donor cornea was removed with a No.15 Bard Parker blade, then the denuded round AM was transplanted onto the corneal surface with the epithelial side up using a #10-0 Nylon (Fig. 1A). A therapeutic bandage contact lens was then applied to protect the epithelium. Postoperatively, 0.3% ofloxacin (four times per day) and artificial tears (frequently) were applied topically until epithelialization was completed. A few weeks later (2-7 weeks), the expanded epithelium with the underlying AM of the donor cornea was harvested with a spatula and crescent knife. This harvest procedure was similar to superficial lamellar keratectomy; however, the stromal dissection was performed at a more superficial layer, under the AM graft. The postoperative management was the same as the in vivo cultivation.
Surgical procedure
To remove fibrovascular tissue from the patient's ocular surface, a superficial lamellar keratectomy was performed with a crescent knife and diamond burr. The cultivated corneal epithelial cell sheet on the AM was transferred onto the corneal surface; it was then sutured with 10-0 nylon. Before the temporary AM graft was covered, epithelial samples were obtained from the donor's cornea at the time of the transplantation procedure; they were then processed for microscopic examination and immunohistochemical staining. Then another AM was applied temporally with the epithelial side down over the cultivated epithelium; 20% autoserum was applied every 2 hr and 0.3% ofloxacin was used four times a day for 2 weeks after surgery.
Microscopic examination and immunohistochemical staining
The peripheral rim of these transplants were partly excised before surgery; they were then prepared for examination by light and JOEL JEM-1200CX transmission electron microscopy. The density of the adhesion complex such as the hemidesmosome, was evaluated as previously described (10). The hemidesmosome density was calculated based on the average of more than 5 points at 40,000 magnification. In addition, immunohistochemical staining was performed in case 1. The monoclonal antibodies against p63 and Integrin β4 were purchased from Santa Cruz (Santa cruz Biotechnology, Santa Cruz, CA, U.S.A.), and the polyclonal antibody against Connexin 43 was purchased from Chemicon (Millipore Corporation, Billerica, MA, U.S.A.). Immunohistochemical staining was performed to evaluate the expression of different molecular markers that have been proposed to identify epithelial basal cells and differentiated cells. In brief, the expanded corneal epithelium were fixed in 2% paraformaldehyde in PBS at 4℃ for 10 min and then permealized with 0.2% TritonX-100 in PBS at room temperature for 10 min. the endogenous peroxidase were quenched with 0.3% H2O2 in 0.5% horse serum in PBS and incubated with 5% horse serum to block the non-specific sites. Monoclonal antibodies against p63 (1:1,000), integrin β4 (1:200), or polyclonal antisera against Connexin 43 (1:200) was applied and incubated for 1 hr at room temperature, followed by incubation with biotinyated second antibodies, anti-mouse or anti-rabbit IgG, using a Vectastain Elite ABC Kit, according to the manfacturer's protocol. The samples were finally incubated with DAB peroxidase substrate to give a brown stain and counterstained with hematoxylin. After washing with PBS, the samples were mounted and analysed.
Evaluation of clinical findings
Epithelial integrity, recurrence of erosion, and decreased size of the PED on the patient's cornea were evaluated postoperatively (1st day, 3rd day, and every week) using slit lamp examination. In addition, the presence of corneal erosion, opacity, and neovascularization on the donor's cornea were evaluated. A clinical success was defined as intact epithelium that was maintained for longer than 4 weeks.
RESULTS
Microscopic findings
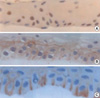
The cultivated epithelial sheet on the donor cornea was well differentiated and multilayered in appearance; they looked normal under the light microscope. They showed markedly stratified epithelia with cuboidal basal epithelial cells and a scanty cytoplasm. The epithelialization on the AM of the donor cornea was completed 2 weeks after expansion. After that time, they showed a well-formed hemidesmosome under the electron microscope (Fig. 1B, C). The calculated hemidesmosome density was 4.3±1.2/2.25 µm, 4.0±1.6/2.25 µm, and 4.2±0.6/2.25 µm at 2, 3, and 7 weeks of culture, respectively.
On immunohistochemical staining of case 1, p63, connexin 43, and integrin β4, were expressed in the epithelial sheet representing well-developed adhesion complexes, intercellular junctions, and the existence of epithelial cells (Fig. 2).
Clinical findings
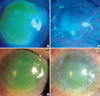
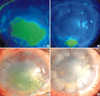
The epithelium that was expanded on the donor cornea was transparent and clear just like normal corneal epithelium. Clinically, the PED of the recipient's cornea was healed with these epithelial sheets (Fig. 3, 4). However, a bandage contact lens was needed to protect the cornea because of its fragility. In detail, the surface of cornea was covered with in vivo expanded epithelium, but a slight small sized erosion was present. The in vivo grown corneal epithelium functioned successfully in all cases; the clinical success rate was 100%. The PED in all cases was covered by 2 weeks after surgery (average 2 weeks). The transplanted epithelium was maintained for 5, 4, and 27 weeks on each of the patient's cornea, respectively (average 12 weeks). The PED recurred in cases 1 and 2 (SJS and severe alkali burn patients). A clear surface was maintained for 27 weeks in case 3, and was followed by a penetrating keratoplasty procedure. The donor cornea recovered completely without any complications at 1 week, 10 days after harvest. Complications such as recurrent erosion, corneal opacity, and neovasculization were not observed.
DISCUSSION
The aim of this study was to evaluate the treatment of PED with total limbal deficiency using in vivo cultivated epithelium. The reconstruction of a severly injured cornea is a challenging problem in ophthalmology. Thus, many experimental methods have been attempted to recover and stabilize the ocular surface prior to performing a penetrating keratoplasty. To date, the limbal autograft or allograft has been most commonly used. However, a variety of obstacles has prevented the clinical success of theses procedures. A limbal autograft requires a large amount of limbal tissue from the healthy eye and is not an option for diseases or injuries that are bilateral. An allograft always carries the risk for rejection and requires patient immunosuppressive treatment for life. As both corneal stem cells and antigen presenting cells (APCs) are transplanted together in limbal allografts, they show intense and frequent rejection. However, very few or almost no APCs are contained in cultivated corneal epithelial sheets ex vivo or in vivo (11).
The most recently used, 'ex vivo' cultivated corneal epithelial transplatation is a very new surgical treatment for severe stem cell deficiency. This new approach has often proven very successful in maintaining good vision in SJS and chemical burn patients (6, 7, 12-14). However, application of this procedure is limited by the facilities and equipment needed. Therefore, in vivo expansion may be preferred to ex vivo expansion.
Previously, we established a well-differentiated multilayered corneal epithelium with adequate hemidesmosome density after 3 months of culture (9). However, this procedure was limited to cell culture of the damanged cornea. Therefore, in this study we investigated corneal epithelium, expanded in vivo in the healthy cornea of living relatives or from the contralateral eye of patients with PED.
Reports have indicated that the prognosis of penetrating keratoplasty (PKP) and limbal transplantation is better in cases where major histocompatibility complex antigens are matched (15, 16). In addition, the antigen-associated blood type is present in corneal epithelial cells (17, 18). Thus, to reduce immune rejection, the cornea from a living relative that is matched for blood type was used for the donor of epithelium in all cases. Epithelialization of in vivo expansion was completed and an adhesion complex like hemidesmosome was present after 2 weeks of expansion, a shorter time than with a damaged cornea.
In vivo expansion on a healthy cornea and donation of the epithelial sheets was a more invasive procedure than a limbal graft. However, the intractable PED did not heal after the limbal graft. The cornea of the donor was completely epithelialized at 7-10 days after the harvest. Complications such as recurrent erosion, corneal opacity, and neovasculization were not observed.
In the three cases with PED, the hemidesmosome density was calculated. They were 4.3±1.2/2.25 µm, 4.0±1.6/2.25 µm, and 4.2±0.6/2.25 µm. They were greater than or equal to the normal value (3.7±60.11/2.25 µm) (19). In addition, immunohistochemical staining results indicated that the epithelial cells were well differentiated and the adhesion complex of epithelial sheets was well developed. These findings showed that corneal epithelia, using in vivo expansion, were well developed after 2 weeks of cultivation. However, integrin β4 was not stained well in the basement membrane, although a well differentiated hemidesmosome was noted. Further studies are needed to better understand the development and differentiation of the hemidesmosome in the in vivo expanded epithelial sheets.
In the case with SJS, the covered epithelial sheet was melted at the fifth week; the epithelial defect along with neovascularization recurred soon after. The cause of this complication might be chronic inflammation, dry eye syndrome, or the toxicity of the eyedrops for chronic dacryocystitis. The patient received two additional expanded epithelium transplantations, ex vivo and in vivo. However, the ocular surface has not improved, and the PED and neovascularization recurred.
In case 2, the patient had severe symblepharon of the eye, and adhesiolysis and AM transplantation on the bulbar and tarsal conjunctiva could not be carried out under ideal conditions. A slightly incomplete eye closure remained, which would contribute to the recurrence of corneal erosion. These finding demonstrate the importance of micro-environmental factors on the ocular surface.
AM is now widely used as an ideal biosubstrate for basement membrane, not only as a surgical material for ocular surface reconstruction, but also an as acellular substrate for tissue engineering (20, 21). In addition, the basement membrane of AM is reported to resemble that of the conjunctival epithelium and closely resembles the basement membrane of corneal epithelium (22). Therefore, preserved AM is considered an appropriate carrier material for the transplantation of cultivated corneal epithelial cells. Moreover, denuded AM has been reported to be more useful than intact AM for the promotion of prompt migration of corneal epithelial cells in vitro and expansion of corneal epithelium (11, 23, 24). Therefore, we used denuded AM as substrate for the basement membrane.
In conclusion, we have described three patients with an epithelial defect of the cornea that was not responsive to standard medical and surgical treatment. We, therefore, introduced a new procedure for transplantation of corneal epithelium, grown in vivo. The PED responded to the in vivo epithelial sheet transplantation. This is the first report on the reconstruction of severely damaged cornea using an epithelial sheet expanded in vivo onto the healthy cornea of a living relative. The results suggest that this approach may be another effective therapeutic option for treatment of PED in severely damaged ocular surface disease.


 XML Download
XML Download