

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of pulmonary disease caused by nontuberculous mycobacteria (NTM) in human immunodeficiency virus (HIV)-negative patients is increasing worldwide (1-5). Lung disease due to NTM occurs commonly in structural lung disease, such as chronic obstructive lung disease, bronchiectasis, and prior tuberculosis. Of the various species of NTM, Mycobacterium avium-intracellulare complex (MAC), M. kansasii, and M. abscessus are the most common causes of NTM lung disease (1, 2).
Unlike M. kansasii lung disease, which is easily treated with conventional anti-tuberculosis drugs, including isoniazid, rifampin, and ethambutol, both MAC lung disease and M. abscessus lung disease are usually resistant to conventional anti-tuberculosis agents. Therefore, these patients have long been considered candidates for surgical treatment when the disease is localized (6-9), and this has been regarded as essential for the treatment of NTM lung disease. The major therapeutic advance in the treatment of NTM lung disease was the introduction of the newer macrolides, clarithromycin and azithromycin, which have substantial in vitro and clinical activity against MAC and M. abscessus. However, many studies have found that pulmonary NTM disease due to MAC or M. abscessus is still difficult to eradicate despite long-term multiple antibiotic therapy, especially in patients with cavitary or bronchiectatic lesions (10-13).
There have been a few reports on the role of surgery in the management of NTM lung disease since the introduction of the newer macrolides. However, they included a substantial proportion of patients who did not receive the recommended standardized combination antibiotic therapy (14-18). Therefore, this study retrospectively examined the outcomes in patients who underwent pulmonary resections for NTM lung disease in recent years while taking the recommended standardized combination antibiotic therapy.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the surgical and medical records of all patients who had underwent pulmonary resection for NTM lung disease at the Samsung Medical Center (a 1,250-bed referral hospital in Seoul, Korea) between January 2002 and January 2007. During this period, 23 patients underwent pulmonary resection for NTM lung disease. Of the 23 patients, 10 patients were identified as having MAC infection (7 with M. intracellulare and 3 with M. avium), 12 patients had M. abscessus infection, and one patient had M. xenopi infection. All the patients met the diagnostic criteria for NTM lung disease, according to the American Thoracic Society (1).
The institutional review board gave permission to retrospectively review and publish the patient records.
Standardized antibiotic regimens
The patients with NTM lung disease were managed according to the guidelines recommended by the American Thoracic Society in 1997 (1).
For treating MAC lung disease, we typically prescribe initial daily dosing with clarithromycin (500 mg twice a day), rifampin (600 mg for body weight >50 kg, 450 mg for body weight ≤50 kg), and ethambutol (25 mg/kg per day for 2 months followed by 15 mg/kg per day). Streptomycin is also used for several months in all patients (1, 4).
The patients with M. abscessus lung disease are treated with clarithromycin (500 mg twice a day), ciprofloxacin (500 mg twice a day), and doxycycline (200 mg twice a day) in combination with parenteral antibiotics, including amikacin (15 mg/kg per day) and cefoxitin (200 mg/kg per day), for the first 4 weeks of hospitalization (1, 4).
Indications for pulmonary resection
Chest computed tomography (CT) was performed preoperatively in all patients to evaluate their lesions, including cavities and bronchiectasis, and underlying pulmonary condition.
Patients were selected for surgery based on consensus by medical and surgical specialists. In general, indications for pulmonary resection included failure of medical therapy, remnant cavitary lesion with a high possibility of relapse, and the development of complications such as massive hemoptysis. Surgical candidates had to have sufficient pulmonary function to tolerate resection and a localized lesion with a high bacterial burden, such as a cavity. For patients with bilateral lesions, the area with the higher bacterial burden was resected, and the remaining lesion with the lower bacterial burden in the ipsilateral or contralateral lung was controlled with medical therapy.
The standard preoperative work-up included chest radiography, chest CT, pulmonary function tests with a quantitative lung perfusion scan, electrocardiogram, echocardiography, and bronchoscopy.
Surgery was performed under general anesthesia using a double-lumen endobronchial tube. The majority of pulmonary resections (16/23, 70%) were performed on the right side. Postoperatively, the patients were scheduled to have intensive antibiotic regimens that were generally same as the preoperative ones. After the sputum acid-fast bacilli (AFB) culture became negative with either medical treatment or surgery, standardized antibiotic therapy was continued for at least 12 months.
Treatment outcomes
Sputum conversion was defined as three consecutive negative sputum cultures tested at monthly intervals. If the patient could not expectorate during the treatment period, the sputum was considered to have converted to negative. The conversion date was recorded as the date of the first negative sputum culture in a patient with negative sputum conversion.
RESULTS
Patient characteristics
During the study period, pulmonary resections for NTM lung disease were performed in 23 patients (7 men and 16 women) ranging in age between 24 and 66 yr (median, 45; interquartile range [IQR], 37 to 57). The main characteristics of the patient population are shown in Table 1. No patients suffered from immunodeficiency disorders such as HIV infection. All the patients underwent lung resection to treat NTM lung disease or the complications of NTM lung disease and not for diagnostic purposes.
The preoperative sputum smear and culture were positive in 15 (65%) and 17 (74%) patients, respectively. All patients had either a cavitary or bronchiectatic lesion on chest CT. The lesions were predominantly cavities in 16 (70%) and predominantly bronchiectasis in seven (30%) patients.
Antibiotic treatment and indication for surgery
A multi-antibiotic regimen based on the standardized protocol for NTM lung infection was initiated preoperatively in 20 patients. The duration of the preoperative antibiotic therapy in these patients was a median of 7.5 months (IQR, 5 to 17; Table 1). Three patients who developed massive hemoptysis did not receive preoperative antibiotic therapy for NTM lung disease.
The indications for surgery included failure of medical treatment in 11 patients (48%), remnant cavitary lesion with a high possibility of relapse in eight patients (35%), and massive hemoptysis in four patients (17%).
In particular, surgery was performed in eight patients who showed some microbiologic improvements (preoperative negative sputum culture in six patients and positive culture in two patients), but had remnant cavitary lesion after antibiotic therapy for a median of 10 months (IQR, 4 to 19). These patients were considered for indication of surgery because of the remnant cavitary lesion with a high probability of relapse. Four patients had MAC lug disease, and four had M. abscessus lung disease. Microscopic findings showed parenchymal destruction with cavity (or multiple cavities) and granulomatous inflammation with caseation necrosis in these patients.
Surgical treatment
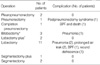
The pulmonary resections included lobectomy in 11 patients, pleuropneumonectomy or pneumonectomy including completion pneumonectomy in four, bilobectomy in three, segmentectomy in three, and lobectomy plus segmentectomy in two patients (Table 2). Nineteen patients underwent open thoracotomy. One patient underwent segmentectomy through a minithoracotomy with video assistance, and three patients underwent video-assisted thoracic surgery without a minithoracotomy (lobectomy in two patients and bilobectomy in one patient). The pathologic findings showed granulomatous inflammation with necrosis in all cases.
The median operating time was 180 min (IQR, 156 to 228 min). The median estimated intraoperative blood loss was 400 mL (IQR, 325 to 575 mL). In nine patients, the blood loss exceeded 500 mL (500 to 4,000 mL), and these patients were given blood transfusions. The median duration of postoperative hospitalization was 9 days (IQR, 6 to 15 days).
Postoperative complications
There were no intraoperative deaths. There was one postoperative death during hospitalization; a 66-yr-old man with M. xenopi lung infection died of respiratory failure associated with the development of a late bronchopleural fistula 47 days after his completion pneumonectomy (19). The right upper lobe had been removed 44 yr earlier for tuberculosis in this patient. There was one late outpatient death; a 44-yr-old man with M. intracellulare lung infection who had been discharged home after an uneventful postoperative course with right upper lobectomy died in an accident 50 days after the operation.
Postoperative complications occurred in eight patients (35%) and included postoperative pneumonia (n=3), late bronchopleural fistula (n=2), prolonged air leak (n=2), wound dehiscence (n=1), and postpneumonectomy syndrome (n=1) (Table 2).
Treatment outcomes
Postoperative antibiotic therapy was administered to 22 patients. In one patient with M. abscessus infection who had bronchiectasis in the right middle lobe and developed massive hemoptysis, neither preoperative nor postoperative antibiotic therapy for M. abscessus infection was prescribed, as there was no residual lesion on chest CT after pulmonary resection.
Negative sputum culture conversion was achieved within 1 or 2 months postoperatively and maintained in all survivors with preoperative culture-positive sputum. Antibiotic treatment was completed in seven patients, who received postoperative antibiotics for a median duration of 12 months (IQR, 6 to 26 months) and were followed up for a median duration of 14 months (IQR, 1 to 22 months) after the end of treatment. In addition, 14 patients received postoperative antibiotic therapy for a median duration of 8 months (IQR, 5.5 to 11 months). Of these 21 patients, no patient has been known to have relapsed during the follow-up period.
DISCUSSION
NTM lung disease has become a significant health problem. However, NTM lung disease remains difficult to treat with medication alone, although the introduction of newer macrolides has improved the outcome of its medical treatment. Therefore, pulmonary resection surgery has been advocated for selected patients who have localized disease and are able to tolerate resection to remove gross lesions that contain large numbers of bacilli (1, 2).
Regarding the treatment of NTM lung disease, the American Thoracic Society has recommended that the initial therapy for patients with MAC lung disease consist of a minimum three-drug regimen of clarithromycin (or azithromycin), rifampin (or rifabutin), and ethambutol (1, 2). In addition, intermittent streptomycin for the first 2 to 3 months of therapy was recommended for extensive disease. Recently, one prospective, randomized trial revealed that a better microbiological response was observed in patients treated with the regimen including streptomycin (20). Nevertheless, the success rates of these medical treatments have peaked at 70-80% (10, 20), and the relapse rate in patients with sputum conversion at the completion of medical treatment is high (21).
For the treatment of M. abscessus lung disease, combined intravenous antibiotic therapy including amikacin and cefoxitin for 2-4 weeks for clinical and microbiologic improvement was recommended in addition to the oral antibiotics, including clarithromycin (or azithromycin) (1). However, the antibiotic treatment of lung disease caused by M. abscessus is usually unsuccessful because of high levels of in vitro resistance, the need for injectable antimicrobial drugs, potentially toxic drugs, and the long treatment duration. Therefore, surgery is usually recommended for patients with localized lung disease who can withstand lung resection after an initial period on antimicrobials to reduce the microbial burden (1, 2, 12, 13).
In our study, all the patients who had received preoperative antibiotic therapy were treated with the recommended standardized regimen. Moreover, streptomycin was routinely administered for several months to patients with MAC lung disease. In addition, the patients with M. abscessus lung disease also received standardized antibiotic therapy, which included 4 weeks of initial intravenous antibiotics while hospitalized. Therefore, the patients included in this study must have received the most effective medication in terms of medical treatment, as compared with those in previous studies (14-18). Nevertheless, the medical treatment outcome was unsatisfactory in our patients.
Therefore, the patients whose disease was mainly localized to one lung and who could tolerate pulmonary resection were considered for surgery. In this study, we were able to assess the surgical outcomes of 23 patients with NTM lung disease. Although most of our patients (n=17, 74%) had preoperative culture-positive sputum for NTM, negative sputum culture conversion was achieved within 1 or 2 months postoperatively and was maintained in all survivors, excluding the two patients who died postoperatively. In addition, no survivor relapsed during the postoperative follow-up period. These results indicate that pulmonary resection can play an important role in achieving a better outcome in selected patients, especially patients in whom medical therapy failed or who had a remnant lesion with a high possibility of relapse.
However, there is no rule concerning the optimal timing of surgery. One retrospective study recommended that patients with localized NTM lung disease be considered for pulmonary resection as early as possible (14). In our study, the median duration of the preoperative antibiotic therapy was 7.5 months, which was shorter than in previous studies (14-18). This was possible because, in recent years at our institution, surgery has been actively considered in patients with localized NTM lung disease when medical treatment appeared ineffective, before the lesions had become inoperable. This treatment strategy may lead to more favorable outcomes. Early surgery with standardized antibiotic therapy may be necessary for patients who are likely to fail medical therapy yet have sufficient predicted postoperative pulmonary function.
Despite the favorable treatment outcomes, postoperative complications were relatively high (35%) with NTM lung disease in our study. This was similar to previous studies that reported a high incidence of postoperative morbidity (14-18, 22, 23).
In conclusion, despite its relatively high surgical complication rate, patients with NTM lung disease whose disease is localized to one lung and who can tolerate resectional surgery might be considered for surgery, if there has been a poor response to drug therapy or if the patients develop significant disease-related complications such as hemoptysis.

 XML Download
XML Download