

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With advances in stabilization devices, surgical techniques, and anesthetic management strategies, multivessel off-pump coronary artery bypass graft surgery (OPCAB) has gained increased popularity worldwide (1, 2). During OPCAB, displacing the heart for exposure of the anastomotic field can elicit a significant hemodynamic deterioration (3, 4). In addition, interruption of the coronary flow for precise vessel anastomosis may result in various degrees of ischemic injury and myocardial dysfunction (3, 5-7).
Various anesthetic and surgical techniques to minimize the myocardial dysfunction and subsequent hemodynamic deterioration have been proposed (3, 5, 8, 9). Among them, insertion of intracoronary shunt has been advocated by many authors with favorable results, which provides bloodless surgical field and some degree of distal flow at the same time (8, 10-12). However, additional technical complexity and intracoronary shunt-induced endothelial damage have raised concerns about the routine use of intracoronary shunt (13-15).
Stenotic lesion of right coronary artery (RCA) in patients with right dominant coronary circulation has been known to be closely associated with right ventricular (RV) function (16-18), which has been suggested as an important prognostic factor of survival (19). Although numerous studies have validated the efficacy of intracoronary shunt on reducing left ventricular dysfunction during OPCAB (8, 10, 11), there is lack of evidence supporting its role on RV function during RCA revascularization. The myocardial dysfunction due to ischemic insult during grafting could be more profound in patients with poor collateral formation (3, 5, 7, 8).
Therefore, we studied the effect of intracoronary shunt on global RV function during off-pump RCA grafting without angiographically visible collateral supply in patients with right dominant coronary circulation using fast-response thermodilution pulmonary artery catheter in a prospective, randomized and controlled trial.
MATERIALS AND METHODS
After approval of Institutional Review Board and patients' consent, 40 patients with either proximal or mid RCA stenosis scheduled for multivessel OPCAB including mid or distal RCA grafting were studied. All patients had right dominant coronary circulation without visible collateral supply to the RCA territory confirmed by preoperative angiography. Patients with preexisting pulmonary disease, left ventricular ejection fraction (LVEF) of less than 40%, and systolic RV pressure of more than 40 mmHg as measured by preoperative transthoracic echocardiography were excluded.
The patients were randomized to RCA revascularization either with intracoronary shunt (Shunt Flo-Thru®, Synovis Surgical Innovations, St. Paul, MN, U.S.A., n=20) or with the proximal RCA occluded by a soft snare (n=20) using a computer-generated randomization table. The anesthesiologists managing the patients were blinded to the randomization results.
All patients received intramuscular premedication (0.05-0.1 mg/kg morphine) 1 hr before operation. Upon arrival at the operating room, standard monitoring devices were applied including a fast-response thermodilution pulmonary artery catheter (Swan-Ganz CCOmbo® CCO/SvO2, Edwards Lifesciences LLC, Irvine, CA, U.S.A.), which was inserted via the right internal jugular vein before induction of anesthesia. The pulmonary artery catheter was positioned in the pulmonary artery using pressure waveform analysis and carefully advanced until pulmonary capillary wedge pressure (PCWP) tracing was obtained. After that, the catheter was connected to an analysis system (Vigilance™, Edwards Lifesciences LLC, Irvine, CA, U.S.A.) and the position of the catheter tip was adjusted to obtain a signal quality index of ≤2 on the analysis system.
Anesthesia was induced with intravenous midazolam (2.0-3.0 mg) and sufentanil (1.5-3.0 µg/kg) and maintained with isoflurane (0.5-1%) and continuous infusion of sufentanil (0.5-1.0 µg/kg/hr). Neuromuscular blockade was achieved by administering rocuronium (0.9 mg/kg) and maintained with continuous infusion of vecuronium (1-2 µg/kg/min). After induction of anesthesia, transesophageal echocardiography probe was inserted in all patients to monitor newly developing segmental wall motion abnormalities. Isosorbide dinitrate 0.5 µg/kg/min was infused in all patients throughout the study period. Diagnostic criteria for post grafting myocardial infarction were new Q waves of greater than 0.04 mm or a reduction in R waves greater than 25% in at least 2 leads, or both, new ST elevation in at least 2 contiguous leads measuring more than 0.2 mV in leads V1-V3 or more than 0.1 mV in all the other leads, or new left bundle branch block (20).
All surgical procedures were performed through a median sternotomy, and the heart was displaced for optimal exposure of the anastomotic field using posterior pericardial stitch, large (12×70 cm) gauze swabs and tissue stabilizer (Octopus Tissue Stabilization System®, Medtronic Inc. Minneapolis, MN, U.S.A.). The sequence of grafting was always the left anterior descending (LAD) coronary artery first, followed by the circumflex coronary artery (LCx) and the RCA. RCA grafting was performed either at the mid or distal RCA in this study. Intracoronary shunt was inserted during all grafting procedures of the left coronary artery.
Intravascular volume replacement was managed with crystalloid and colloid solutions to maintain the PCWP between 8-14 mmHg before first grafting. During the period of heart displacement, mean systemic arterial pressure (MAP) was maintained above 70 mmHg either with 10-20° Tredelenburg position and/or norepinephrine infusion.
Hemodynamic variables including heart rate (HR), MAP, central venous pressure (CVP), mean pulmonary arterial pressure (MPAP), PCWP, cardiac index (CI), mixed venous oxygen saturation (SvO2), RV end diastolic volume index (RVEDVI), and RVEF were recorded 15 min after returning the heart to its natural position following completion of grafting at the left coronary arteries before RCA grafting (baseline, T1), 10 min after application of tissue stabilizer for distal anastomosis of the RCA (T2), and 15 min after completion of RCA grafting with the heart in its natural position (T3). The amount of infused norepinephrine at T2 and the total amount of infused fluid throughout the study period were also recorded. Corresponding pulmonary vascular resistance index (PVRI) and RV stroke work index (RVSWI) were calculated.
Statistical analyses were performed using SPSS 12.0 (SPSS Inc., Chicago, IL, U.S.A.). We determined that 17 patients would be required in each group with 80% power to detect a 5% difference in RVEF between the groups with a standard deviation (SD) of 5% and an alpha level of 0.05 using independent t-test. All data are expressed as the number of patients or mean±SD. Data between the groups were compared using chi-square test, Fisher's exact test, or independent t-test as appropriate. Changes between time points within the groups were compared using univariate analysis of variance with post hoc comparison using Dunnette's test. A p value of less than 0.05 was considered statistically significant.
RESULTS
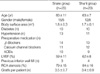
Patients' characteristics were similar between the groups including preoperative LVEF and percentage of RCA stenosis (Table 1). OPCAB could be successfully performed in all patients without any occurrence of dangerous arrhythmia requiring prompt treatment or conversion to cardiopulmonary bypass during RCA grafting. There were no newly developed segmental wall motion abnormalities or ECG changes indicative of myocardial infarction after grafting.
None of the patients required intraoperative inotropic support and the amount of infused norepinephrine during RCA grafting was similar between the groups (snare group, 71±49 µg; shunt group, 65±47 µg). The time required for RCA grafting was similar between the groups (snare group, 15.4±1.3 min; shunt group, 16.1±1.2 min). The total amount of infused fluid during the surgery was also similar between the groups (snare group, 3,923±876 mL; shunt group, 4,063±737 mL).
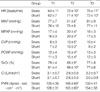
In intergroup comparisons, there were no significant differences of the hemodynamic variables except the MAP, which was higher in the snare group during RCA grafting (p=0.021, Table 2).
In intragroup comparisons, HR, MPAP, CVP, PCWP, and PVRI were significantly increased in both groups during RCA grafting compared to baseline values of each group, but returned to baseline values at T3 except HR (Table 2). SvO2, RVEF, and RVSWI were significantly decreased in both groups during RCA grafting compared to baseline values of each group, but returned to baseline values at T3 (Table 2, 3). Other variables did not show any significant changes compared to baseline values (Table 2, 3).
DISCUSSION
In this study, we evaluated the effect of intracoronary shunt during RCA anastomosis on global RV function in patients theoretically vulnerable to ischemia-induced RV dysfunction during RCA grafting with extraluminal coronary occlusion. Insertion of intracoronary shunt was not associated with any positive effects on global RV function in terms of RVEF and RVSWI during RCA grafting. In both groups, RVEF and RVSWI decreased compared to baseline values during RCA grafting and returned to baseline values after reperfusion.
Favorable results have been reported supporting the use of intracoronary shunt during LAD grafting regarding global as well as segmental LV function and reduced postoperative troponin I level (8, 10-12). However, brief periods of extraluminal coronary occlusion are generally well tolerated in most patients, and evidence of intracoronary shunt-induced endothelial damage that was not found with extraluminal coronary occlusion with soft snare, has been reported raising concerns about long-term graft patency (13-15). Therefore, insertion of intracoronary shunt was recommended in selective cases with severe, multivessel coronary disease and poor cardiac function or poor collateral formation (8, 10, 12, 13).
RV failure is being increasingly recognized as an important cause of perioperative morbidity, and global RV function is predominantly determined by the RV free wall, which is primarily supplied by the RV branches (16, 17, 19). We have enrolled patients undergoing mid or distal RCA revascularization where coronary hemostasis with soft snare could impair flow to the RV branches as well as acute marginal and posterior descending branches. In addition, all of our patients had right dominant coronary circulation without angiographically visible collateral formation where the RV receives its blood supply almost exclusively from the RCA. Therefore, the effect of intracoronary shunt in minimizing global RV dysfunction was assumed to be significant in this study.
In contrast to the above-mentioned favorable results regarding the LV function with insertion of intracoronary shunt during LAD grafting (8, 10-12), we could not observe a significant difference in global RV function. During RCA grafting, the heart is displaced more, resulting in greater alteration of the normal geometry than during LAD grafting (3, 4). The subsequent increase in RV afterload, which could be observed as increase in PVRI in both groups in this study, could have offset the potentially favorable effect of intracoronary shunt insertion on global RV function. Under normal conditions, RV function is load-dependent, and even though RVEDVI remained constant in this study, abnormally increased afterload becomes the major determinant of the RV function (21). Also, prior grafting of the LAD could have affected our result. Since the LAD supplies part of the RV anterior wall (16), this could have supported RV function during RCA grafting, although global RV function is predominantly determined by the RV free wall (16, 17). In addition, prior LAD and LCx revascularization might have resulted in improved recruitable collateral flow to RCA territories.
Ischemia-related transient segment wall motion abnormalities of the RV during RCA grafting could have developed in the snare group, which was unable to detect with the fast-response thermodilution pulmonary artery catheter. Unlike the diagnosis of ischemia-related segmental wall motion abnormalities in the LV, measurement of RV contractility and segmental wall motion is difficult with TEE because of the complex shape of the RV and is especially limited during OPCAB when the heart is displaced from its original position (3, 22, 23). The fast-response thermodilution pulmonary artery catheter continuously measures RVEF by a thermodilution technique, which has a high reproducibility and a good correlation with other methods of measurement (22-24). The observations that RVEF and RVSWI returned to baseline values after reperfusion and that none of our patients showed newly developed segmental wall motion abnormalities or ECG changes indicative of myocardial infarction afterwards indicate no clinically beneficial effect by intracoronary shunt insertion with regard to ischemia-related RV function.
Limitations of this study are as follows. Occurrence of serious arrhythmia and/or hemodynamic collapse requiring immediate cardiopulmonary bypass has been reported during RCA grafting, especially when the atrioventricular (AV) nodal artery flow is interrupted (3, 6). Although AV node is supplied by the RCA in 80% of normal human hearts, the remaining 20% receives its blood supply either by the LCx or both LCx and RCA (25). In addition, all of the patients in our study tolerated well with extraluminal coronary occlusion and the incidence of such critical event is very low (6). Therefore, in order to validate the safety of the extraluminal coronary occlusion with regard to serious arrhythmia, further studies with a larger number of patients are warranted.
Another limitation of this study is that collaterals visualized on preoperative angiography may not reflect accurately the total collateral flow and recruitable collaterals might have existed (26). The result that MAP was significantly higher during RCA grafting in the snare group might have resulted in better recruitable collateral flow. However, MAP was maintained above 70 mmHg in both groups during RCA grafting and the effect of difference in MAP on recruitable collateral flow should be negligible.
To avoid distorting the comparative study outcome, we have excluded patients with decreased LVEF and systolic RV pressure ≥40 mmHg who could be more susceptible to ischemia-induced RV dysfunction, and the results of our study should not be extended to these patients.
In conclusion, we could not observe beneficial effects with intracoronary shunt insertion compared to temporary extraluminal coronary occlusion with regard to global RV function during RCA grafting even in ischemia-susceptible patients without angiographically visible collateral formation. Regarding the possibility of long-term graft failure by intracoronary shunt-induced endothelial damage, routine use of intracoronary shunt during RCA grafting in patients with preserved biventricular function is not recommended.

 XML Download
XML Download