

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The disease process of atherosclerosis begins in childhood. In an autopsy study, fatty steaks were found in the aortas of children older than 3 yr and in the coronary arteries by adolescence (1). Although cardiovascular morbidity is rare during children as a result of hypertension, many researches suggest that sequelae of hypertension such as left ventricular hypertrophy and diastolic ventricular dysfunction begin years of decades before the onset of coronary artery disease and stroke.
In adults, non-invasive ultrasonographic assessment of large arteries and increased intima-media thickness (IMT) of the carotid artery (cIMT) have been shown to correlate with cardiovascular risk in hypertensive patients (2, 3). Increased cIMT has also been reported in diabetic children (4), children with familial hypercholesterolemia (5), growth hormone deficiency (6), William syndrome (7), and Kawasaki disease (8), compared with normal controls. However, there are few studies on the correlation between cIMT and cardiovascular risk in hypertensive children. Although the ultrasound method for measuring cIMT does not allow for differentiation of intimal atherosclerosis from medial hypertrophy due to pressure effects, increased cIMT is well established as a marker for cardiovascular risk in adults. Recently, studies suggested that IMT represents an early manifestation of vasculopathy in children.
Pulse wave velocity (PWV), another non-invasive method measuring arterial stiffness, has been noted as a useful method of evaluating the severity of atherosclerosis in adults (9). Recently, a novel device that measures brachial-ankle PWV (ba PWV) was developed. The validity and reproducibility of baPWV measurements were reported in adults and the method seemed to be an acceptable marker reflecting vascular damage.
A relationship between aortic stiffness and hypertension (10) has also been noted in children. Only limited data on PWV in hypertensive children have been reported.
The purpose of this study was to investigate whether IMT and PWV are useful diagnostic markers in predicting early atherosclerosis in adolescents with essential hypertension.
MATERIALS AND METHODS
Patients
Fifteen hypertensive patients (14 male and 1 female) and 17 normotensive subjects (12 male and 5 females), aged between 16-18 yr, were involved in the study.
The hypertensive adolescents were recruited from the middle and high school students screened for hypertension. They were newly diagnosed patients who were diagnosed as essential hypertension subsequently. We only included whose systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg. Elevated blood pressure was confirmed in a pediatric clinic by averaging the 3 blood pressure measurements made after 5 min of rest with an oscillometric monitor.
Informed consent was obtained from the parents and study participants.
Bioelectrical impedance analysis
Measurements were made with a segmental bioelectrical impedance analyzer, using eight tactile electrodes according to the manufacturer's instructions (InBody 3.0; Biospace, Seoul, Korea). A pair of electrodes was in placed on the surface of each hand and foot and hand. These electrodes were connected to current and voltage terminals from an impedance meter via electronic on/off switches, which were regulated by a microprocessor. The target segment could be measured selectively.
Intima-media thickness of common carotid artery
The same investigator performed non-invasive measurements on the carotid artery using a real-time B-mode ultrasound imager (iU22, intelligent Ultrasound System; Philips, Amsterdam, Netherlands) and a probe of 12.5 MHz. For all subjects, the IMT and lumen diameter were measured in the same arterial segment.
The measurements were performed within 1 cm above the bifurcation of the right common carotid artery. The IMT of artery was defined as the distance between two parallel echogenic (bright) lines of the vessel in the sonography. The first line near the lumen is the intimal-luminal interface, and the second one, close to the adventitia, is produced by the collagen containing the upper layer of the tunica adventitia. IMT, lumen diastolic (dD), and systolic diameters (sD) were measured in the anteroposterior projection with the patient lying supine, after at least 30 min of recombent position.
The measurements were substituted for calculation according to the following formulae described by Aggoun et al. (11).
Lumen cross-sectional area=πdD2/4
Wall cross-sectional area=π(dD/2+IMT)2-π(dD/2)2.
Cross-sectional compliance=[π(sD2-dD2)]/4△P (mm2.mmHg-1)
Cross-sectional distensibility=(sD2-dD2)/(dD2△P)(mmHg-1.10-2)
△P: pulse pressure
Pulse wave velocity
baPWV was measured in supine position by VP-1000 (Colin Co., Komaki, Japan). Using volume plethysmographic technique, PWV, ABI (Ankle brachial index, the ratio of systolic blood pressure in the ankle to that in the brachial artery), blood pressure, electrocardiography and pulse were obtained simultaneously. Sphygmomanometer cuffs were wrapped on both the brachia and ankles, electrocardiogram electrodes were placed on both wrists, and a microphone was placed on the left edge of the sternum. As the pulse wave contours in the four extremities were recorded, the cuffs inflated and deflated automatically. Pulse transit time between the brachial and ankle regions was computed from these pulse volume recordings. baPWV was determined from the pulse transit time and the distance between these two segments. The distance of each segment was calculated automatically, based on the height of the subjects.
Lipid profile
Blood samples were taken from venous puncture after midnight fasting. The following laboratory studies were performed in all subjects and controls: fasting lipids levels [total, low-density lipoprotein (LDL)-, high-density lipoprotein (HDL)-cholesterol, and triglycerides], plasma homocysteine, insulin, aldosterone, renin and angiotensin converting enzyme (ACE).
The plasma cholesterol concentration was measured with an enzymatic colorimetry (ADVIA 1650; Bayer, Pennsylvania, U.S.A.) and triglyceride concentrations were measured with an enzymatic method.
Homocysteine, insulin, Vit B12 and folate
Plasma homocysteine was measured by automated Bayer ADVIA Centaur chemiluminescent Hcy assay. Insulin was determined using radio-immunoassay (RIA) commercially available kit by Biosource, Belgium with Gamma counter (Hewlett Packard, California, U.S.A.).
Plasma concentrations of vitamin B12 and folate were quantified with a radioassay Gamma Counter (Packard, California, U.S.A.).
Renin, aldosterone and ACE
Plasma renin and aldosterone were measured with COBRA-II Gamma counter (Packard, California, U.S.A.). Blood samples for renin concentration were taken after 30 min supine rest and measured directly by an improved immunoradiometric assay.
Statistical analysis
All statistical analyses were done with SAS system (Windows version 11.0).
Descriptive statistics were presented as percentages, means, and standard deviations. Univariate analyses for group comparisons of continuous variables were performed using student t-test.
The correlations among continuous variables were determined using the Pearson correlation coefficient. A p value less than 0.05 was regarded as significant.
RESULTS
The majority of subjects in the study were male (87.5%). Sixty percent of hypertensive adolescents and 17% of control were obese, defined as BMI ≥95th percentile for age and gender. Hypertensive subjects had significantly higher weight, height, BMI, obesity index, arm circumference, fat mass, fat distribution and systolic blood pressure as shown in Table1.
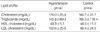
Among 15 hypertensive adolescents, 12 (80%) had isolated systolic hypertension, and 3 (20%) had both systolic and diastolic hypertension. There was no significant difference in the mean of serum lipid level between two groups (Table 2).
Hypertensive adolescents had significantly greater values of cIMT (0.62±0.013 mm vs. 0.50±0.010 mm) (p<0.05) than normotensive children. Elastic properties such as cross-sectional compliance (0.15±0.04 mm2/mmHg vs. 0.23± 0.10 mm2/mmHg) and distensibility (0.0053±0.0021 mmHg-1/10-2 vs. 0.0087±0.0045 mmHg-1/10-2) of the carotid artery were also significantly different between hypertensive and normotensive group (p<0.05) (Table 3).
Several biochemical indices which are known to be related to hypertension and coronary disease were compared. Serum homocysteine, folate, insulin and vitamin B12 were measured. Only vitamin B12 level showed significant decrease (551.5±251.7 pg/mL vs. 859.8±454.4 pg/mL ) in hypertensive group (p<0.05) (Table 4).
Renin, aldosterone and ACE levels were also measured and no significant difference was observed in our study (Table 5).
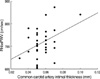
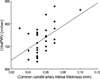
PWV were measured separately for the comparison. Right heart brachial-ankle pulse wave velocity (RhbaPWV) and left heart brachial-ankle pulse wave velocity (LhbaPWV) of hypertensive group were 745.9±63.2 cm/sec and 759.2±60.8 cm/sec respectively, which were significantly increased compare to normal control (p<0.05) whose average values were 690.6±56.0 cm/sec and 702.6±51.5 cm/sec for right and left side of the body (Table 6). There was significant correlation between the hbaPWV and IMT (Fig. 1, 2).
DISCUSSION
Hypertension is one of the leading factors for the development of atherosclerosis. Although serious morbidity occurs rarely, essential hypertension starts to develop in childhood. Some end organ complications are also reported in children. Left ventricular hypertrophy and retinal hypertensive angiopathy are observed (12). Impaired left ventricular relaxation, left ventricular remodeling, and a high prevalence of left ventricular hypertrophy are reported as a result of the diastolic dysfunction of hypertensive children (13).
Noninvasive tests such as carotid artery B-mode ultrasound, PWV, ankle brachial blood pressure ratios, carotid artery duplex scanning, electron beam-computed tomography, ultrasound-based endothelial function studies and magnetic resonance imaging techniques offer the potential method for measuring and monitoring atherosclerosis.
IMT of large artery walls, especially carotid, can be assessed by B-mode ultrasound in a relatively simple way and represents a safe, inexpensive, precise and reproducible measure (14). Recent studies have suggested that preclinical hypertensive sequelae may also be detected by the use of vascular ultrasonography. In adults, increased IMT of the carotid artery has been shown to indicate the presence of atherosclerosis and predict cardiovascular morbidity and mortality (15).
Since carotid IMT is a marker of early arterial wall change, including atherosclerosis and/or vascular hypertrophy, its detection by B-mode ultrasonography might participate in the diagnosis of high cardiovascular risk and in the decision to treat aggressively those patients at risk with drug treatments (16). Studies in adults with hypertension have shown that IMT in common carotid arteries correlates with cardiovascular risk and the severity of hypertension (17). Before proposing the routine measurement of IMT in clinical practice several limitations have to be overcome such as the standardization of methods of measurement including the site and the analysis of the measurement and a precise definition of the threshold of IMT (18).
Increased IMT is regarded as one of the first signs of early atherosclerosis in adult. There are few reports that have indicated a correlation between cIMT and hypertension in children (19). Recently, Sorof et al. (20) reported significantly increased cIMT in hypertensive compared with healthy children.
We found that hypertension is accompanied by greater IMT and diminished elasticity of the carotid artery. Such changes are visible in childhood. In a recent study of Sorof et al. (20) carotid IMT was correlated with BMI, age, height, and weight in groups of healthy and hypertensive children. But significant correlation was not noted between carotid IMT and BMI or weight in this study. Mechanical properties of the arterial wall, including distensibility, compliance were also deranged in hypertensive children.
Some studies of hypertensive adults have reported an increased lumen diameter of the common carotid artery and an increase in the IMT to lumen ratio (21). Distensibility is inversely correlated with pulse pressure and this variable was significantly greater in the hypertensive group (12). In our study, decreased distensibility and compliance were noted in hypertensive adolescents. The reduction of artery wall distensibility and compliance of the elastic arteries in essential hypertension is still incompletely understood. But it is suggested by the increase in blood pressure or intrinsic changes in the wall.
Essential hypertension must last sufficiently long to cause remodeling of the arterial wall, which will further reduce compliance of the artery. The incremental elastic modulus of the artery is independent of the lumen diameters and reflects the elastic properties of the arterial wall. Increased IMT may be related not only to hypertension, but also to other factors damaging the vascular wall, such as homocysteine or lipids (12). However, in our study there was no significant change of serum lipid and or homocysteine levels in hypertensive children compared with control group. Renin, aldosteron, ACE level were not different between two groups except vitamin B12 level.
Recently, PWV has been noted as a simple, non-invasive, and automatic method for evaluating arterial stiffness, which is strongly associated with systemic atherosclerosis at various sites in the vascular tree (22, 23). Measurement of carotid-femoral PWV is recognized as an established method to evaluate the severity of atherosclerosis and predictor of cardiovascular mortality in adults. The recently published study by Dernellis and Panaretou provided evidence that increased aortic stiffness precedes hypertension (24). They suggested that the alteration in arterial function is present already in nonhypertensive subjects at risk of hypertension and it may contribute to the progression to hypertension in later life (24). BaPWV would be essential for the screening of atherosclerosis in children.
There are very few reports on the influence of age and gender on arterial stiffness or reference value in healthy children (25). Since arterial stiffness is greatly influenced by age and gender. It is certainly necessary to evaluate the influence of age and gender on baPWV. Further, it has been shown that, in adults, baPWV is strongly influenced by gender, and that baPWV is higher in men than in women (26). In our previous study, baPWV was higher in normotensive male adolescents compared with female adolescents (27). In our previous report, a positive correlation was found between the systolic, diastolic, average blood pressure and PWV (28). This is because blood pressure directly affects pulse waves, and structural changes due to chronic hypertension increase PWV, in addition, stiffness of arterial walls itself affects blood pressure. In this our study, the carotid IMT and baPWV were significantly higher in hypertensive adolescents compared with normal control. And also, the carotid IMT significantly correlated with baPWV in hypertensive adolescents.
In our result, we found that hypertension is accompanied by greater IMT and diminished elasticity and distensibility in childhood. The differences between hypertensive and healthy children were highly significant although values of IMT in our patients were much lower than those reported in adults. However, there are no data on any cut-off value of carotid IMT in childhood, as an index of increased risk of cardiovascular events in adolescents.
There were several limitations in this study. This study was a small scale investigation including only 15 adolescents as subjects. Since arterial stiffness is greatly influenced by age and gender, it is certainly necessary to evaluate the influence of age and gender on baPWV. However we did not evaluate arterial stiffness according to age and gender.
In conclusion, we report that in children with essential arterial hypertension there is evidence of subclinical arterial damage i.e. endothelial dysfunction, changes in thickness, distensibilitiy and compliance of arterial wall. This causes not only an increase in IMT of the arterial wall but also a significant decrease in the elastic properties of the artery. Our results suggest that carotid IMT and PWV may be useful for predicting coronary artery disease and other cardiovascular sequale in hypertensive children. A larger scale investigation should promise more reliable results about carotid IMT and PWV in hypertensive adolescents.





 XML Download
XML Download