

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Elevated intraocular pressure (IOP) is one of the major risk nfactors for glaucomatous visual field defects. In addition, it is associated with various systemic diseases and indices (1-6). Each systemic risk factor of coronary heart disease (CHD) has been associated with an elevated IOP, including hypertension, male gender, a high body mass index (BMI), and hyperlipidemia (7, 8). However, no reports have argued for a correlation between the risk factors for CHD including smoking, low-density lipoprotein (LDL)-cholesterol, and triglyceride and IOP after a comprehensive or collective analysis. The National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) developed the Framingham projection, which can predict the risk of CHD quantitatively. The Framingham projection is an index that predicts the probability of having a CHD event within 10 yr. No reports have analyzed the relationship between IOP and the Framingham projection, which incorporates all the risk factors for CHD (2, 5, 7, 9). Therefore, we investigated the association between IOP and cardiovascular risk factors and between IOP and the Framingham projection in 16,383 Korean subjects.
MATERIALS AND METHODS
The study subjects were 16,383 adults from 20 to 79 yr old who visited the Health Promotion Center of Asan Medical Center from July to December of 2001. There were 9,795 men and 6,588 women. The mean age of the men and women was 46.5 and 46.1 yr, respectively. Sixty-five percent of the subjects lived in Seoul and had regular check-ups and subsequent consultations concerning diet and exercise if needed. The body mass index (BMI=weight divided by the height squared), blood pressure, smoking history, total cholesterol, triglycerides, high-density lipoprotein (HDL)-cholesterol, LDL-cholesterol, and high sensitive C-reactive protein (hs-CRP) were measured. Blood samples were taken in the morning after fasting for more than 9 hr. The serum total cholesterol, triglyceride, and HDL-cholesterol concentrations were measured using enzymatic methods on a Hitachi 747-200 (Hitachi, Tokyo, Japan). The serum LDL-cholesterol concentration was calculated using the Friedewald formula (10). The hs-CRP concentration was measured using immunoturbidimetry on a Cobas Integra 800 (Roche Diagnostic System, Basel, Switzerland). Applying the Framingham projection, the 10-yr absolute CHD risk (i.e., the percent probability of having a CHD event within 10 yr) was calculated using age, total cholesterol, cigarette smoking, HDL-cholesterol, and systolic blood pressure. The IOP was determined as the mean value of the readings for both eyes using a non-contact tonometer (T-2, Canon, Tokyo, Japan) between 9 and 11 a.m.
Statistics
Student's t-test was used to determine the statistical difference between men and women in the mean of each factor. Parametric correlation analyses were used to analyze the statistical significance between the Framingham projection and IOP and between each risk factor and IOP in both men and women. After correcting for the other risk factors, stepwise multiple linear regressions were performed to determine if each risk factor affected the mean IOP independently. The mean IOP was compared between the high- (10-yr risk > 20%) and low-risk (10-yr risk ≤ 20%) CHD groups based on the Framingham projection. The software SPSS (version 11.0, SPSS Inc., Chicago, IL, U.S.A.) was used for the statistical analyses.
RESULTS
Comparison of IOP and the Framingham projection between men and women
The mean IOP (men 12.3±3.1 mmHg, women 11.8±2.6 mmHg) and the Framingham projection (men 8.7±4.8, women 6.7±6.6) were significantly higher in men than in women (p < 0.05). Men were significantly older, smoked more, and had higher systolic blood pressure, triglycerides, LDL-cholesterol, total cholesterol, and hs-CRP than women, and significantly lower HDL-cholesterol (p < 0.05; Table 1).
Correlation between IOP and other parameters
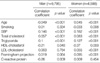
In men, the mean IOP had significant negative correlations with age, HDL-cholesterol, and hs-CRP and positive correlations with systolic blood pressure, total cholesterol, and triglycerides (p < 0.05). Nevertheless, the mean IOP was not significantly correlated with the Framingham projection. In women, the mean IOP had significant negative correlations with smoking and HDL-cholesterol and positive correlations with age, systolic blood pressure, total cholesterol, triglycerides, and LDL-cholesterol (p < 0.05). Moreover, the mean IOP had a significant positive correlation with the Framingham projection (p < 0.05; Table 2).
Stepwise multiple regression for correlated factors
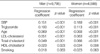
After correcting for the other risk factors in men and women, the following were independent risk factors that were related to an elevated IOP in descending order: in men, increased systolic blood pressure, triglycerides, LDL-cholesterol, and total cholesterol, decreased HDL-cholesterol, and age (p < 0.05); in women, increased systolic blood pressure, triglycerides, total cholesterol, and LDL-cholesterol, decreased HDL-cholesterol, and age (p < 0.05; Table 3). In both men and women, the mean IOP of the high-risk CHD group (men 12.7 mmHg, women 13.7 mmHg) was higher than that of the low-risk CHD group (men 12.2 mmHg, women 11.8 mmHg; p < 0.05).
DISCUSSION
The mean IOP in men (12.3±3.1 mmHg) was higher than that in women (11.8±2.6 mmHg), which agreed with previous reports for Korea (11, 12). This was because the increases in systolic blood pressure, total cholesterol, triglycerides, and LDL-cholesterol and the decrease in HDL-cholesterol, which were factors that influenced the IOP, were much more prominent in men than in women. In contrast, some studies involving other ethnic groups found that the mean IOP in women was higher than that in men (13).
After correcting for all systemic health parameters, the mean IOP decreased as age increased in both sexes, which was consistent with previous reports for Korea and Japan (7, 11). By contrast, in Westerners, even after this correction, the IOP increased with age (13). Ethnic differences may arise because as Orientals grow older, they are less prone to increases in blood pressure, blood lipid concentrations, and obesity than are Westerners. Age had a less effect on the Framingham projections than the other risk factors. The mean IOP in the high-risk CHD group based on the Framingham projections was higher than that of the low-risk group.
Of the risk factors contributing to the Framingham projection, i.e., age, total cholesterol, cigarette smoking, HDL-cholesterol, and systolic blood pressure (BP), the increase in systolic BP had the greatest independent relation to elevated IOP. The association between the increase in the systolic BP and the elevated IOP agreed with previous reports (8, 9). High BP increases the pressure in the ciliary artery and the ultrafiltration component leading to formation of the aqueous humor, thereby increasing the IOP.
We could find a significant association between diabetes, which is not included in the Framingham projection, and elevated IOP (diabetic group [n=2,053]: 12.3±3.2 mmHg, non-diabetic group [n=14,330]: 12.0±2.9 mmHg, p < 0.05). This is consistent with a previous report that diabetes was related with an elevation in IOP (5).
Most of the previous studies used only total cholesterol as the serum lipid marker (14), and some could not show a direct association with an elevated IOP (9). Of the lipid markers, triglycerides, not a component of the Framingham projection, had the greatest relation with the elevated IOP based on the regression coefficients. In addition to total cholesterol and HDL-cholesterol, both of which contribute to the Framingham projection, LDL-cholesterol and triglycerides were independent risk factors of an elevated IOP. These prominent findings strongly support the role of the serum lipid markers in IOP elevation. The increase in blood viscosity and decrease in outflow channel capacity due to hyperlipidemia contribute to the elevation in IOP. We added LDL-cholesterol and triglycerides, CHD risk factors emphasized by NCEPATP III, to the Framingham projection to make a new predictor for IOP elevation.
An increase in total cholesterol and decrease in HDL-cholesterol are high-risk CHD factors that increased the Framingham projection and were both independent risk factors for increasing IOP. Several reports support our results in that hyperlipidemia, which is strongly related to obesity and an increased BMI, was associated with elevated IOP (11, 14).
We could not find any direct significant association between smoking and elevated IOP, even after correcting for the other risk factors. This contrasts with a previous report that smoking was associated with an elevation in IOP, but those studies did not correct for other risk factors and the mechanism of IOP elevation is still not clear (2, 15, 16). Although the Framingham projection includes smoking as one of the main risk factors of CHD, smoking had little relation to IOP elevation.
The mean IOP was significantly higher in the high-risk CHD group (men 12.7 mmHg and women 13.7 mmHg) than in the low-risk CHD group (men 12.2 mmHg and women 11.8 mmHg), when the risk of CHD was based on the Framingham projection. The high-risk CHD group was defined as a 10-yr risk of over 20%, i.e., the Framingham projection was over 16 points in men and over 23 points in women. In terms of systemic parameters that describe or reflect elevation in IOP, the Framingham projection, a major predictor of CHD, best predicted elevation in IOP. In particular, the increase in the Framingham projection due to the increased systolic BP and total cholesterol and decreased HDL-cholesterol best reflects the elevation in IOP. Therefore, we recommend that these parameters be monitored along with regular IOP measurements.
In conclusion, elevated IOP is associated with cardiovascular risk factors. Young age, high systolic BP, total cholesterol, triglycerides, LDL-cholesterol, and low HDL-cholesterol were independent risk factors for elevation in IOP. Therefore, subjects with a high risk of CHD based on the Framingham projection need continuous monitoring for IOP to prevent glaucomatous visual field defects.

 XML Download
XML Download